Too Much or Not Enough of a Good Thing?:
Reconciling Differing Perspectives on the Optimal Dose of Mindfulness Meditation and Advancing a Dose-Response Research Agenda
Keywords: mindfulness, meditation, dose response, Buddhism, optimization
Abstract: Mindfulness meditation is now practiced broadly in both religious and secular contexts, with numerous studies indicating potential benefits across a range of psychosocial domains. However, despite significant research effort, we still know little about dose-response effects—how frequently or for how long individuals might need to practice mindfulness meditation to achieve certain practice goals. Increasingly, recommended amounts of practice are becoming shorter, with unclear effects on outcomes. We review and critically appraise the state of knowledge about dose-response effects drawn from empirical investigations, traditional sources, and trends in contemporary teaching and practice. We argue that limitations inherent to the range of doses and analytic approaches used in previous studies reduce our ability to inform the dose-response question. We propose a practical research agenda that prioritizes the question of dose response, incorporating design features optimized specifically to understand the dose-response relationship and how it might vary between outcomes and individuals. Prioritizing the dose-response agenda will allow us to reconcile differences between knowledge sources and enable us to optimize mindfulness programs based on individuals, their goals, and the context in which they practice.
Introduction
Mindfulness meditation has experienced a meteoric rise in popularity over the past several decades. In 2022, almost one in five US adults (18.3 percent) reported having meditated (including mindfulness as well as spiritual and mantra meditation), a twofold increase from 2002.[2] Estimates from a weighted representative sample in the United Kingdom suggest similar rates.[3] From its roots in ancient religious traditions, notably Buddhism, where mindfulness was typically practiced toward soteriological transcendent goals, secular mindfulness practice has been widely adopted and repackaged within mainstream healthcare and wellness industries to promote physical, mental, and spiritual wellbeing.[4] In line with this historical trajectory, mindfulness meditation herein will serve as an umbrella term representing a collection of attitudinal and attentional practices that have inspired and formed the basis of mindfulness-based programs (MBPs),[5] including mindfulness-based stress reduction (MBSR).[6]
Since MBSR was developed in the late 1970s, a plethora of MBPs have followed, catering to individuals with wide-ranging backgrounds, goals, and commitment levels. The scientific study of mindfulness meditation has largely focused on variation in the content of these MBPs, though more recently there has been an increased focus on digital adaptations that are typically shorter and less intensive, along with being delivered at a greater scale.[7] Meta-analyses have identified modest psychosocial benefits across in-person, teacher-led programs with varying lengths and intensities but with a minimum of four hours of instruction.[8] The evidence regarding the efficacy of shorter and/or digital programs is much weaker,[9] and these programs have suffered from high attrition and low user engagement over time.[10]
Despite an evidence base exceeding 2,500 randomized controlled trials, according to PubMed as of September 2025, we still know very little about how frequently or how long individuals might need to practice mindfulness meditation to achieve specific practice goals. That is, we know virtually nothing about dose-response effects for mindfulness meditation, defined here as the relationship between the length and/or frequency of formal practice sessions, and the cumulative amount of practice needed over time to see meaningful effects across the range of outcomes toward which individuals are striving. Where empirical work fails to distinguish between the effects of smaller and larger doses, authors have suggested that smaller doses may be sufficient.[11] This conclusion clashes with the expert opinions of mindfulness teachers, who almost universally emphasize the benefits of longer practice sessions, as we outline below. We argue that the absence of evidence is not evidence of absence, and that alternative methods or statistical approaches can better inform such potential conclusions.
Best practice behooves us to build evidence that can help inform guidelines that beginner meditators and their health, wellbeing, or spiritual advisers can use to estimate the time and effort required to achieve a particular goal. Dose recommendations can then be tailored to individual needs based on various factors, including a person’s medical and psychological history, personality type, and life circumstances. The current evidence base fails to achieve this because insufficient research has been conducted, and the methodological approaches used so far have been ill-equipped for this purpose. Herein, we suggest a path forward for empirical dose-response investigations regarding the length and frequency of formal mindfulness meditation practice sessions (and their combination—i.e., cumulative practice time).
Limitations of Existing Empirical Dose-Response Investigations
The lack of support for the dose-response hypothesis is, in our view, due to the paucity of well-designed studies optimized for this purpose. We know of only four empirical studies that have experimentally manipulated session duration to explicitly test for dose-response effects with mental health or wellbeing measures. In the first, there was no difference in effect between practicing ten or twenty minutes daily over a two-week period for psychiatric symptoms.[12] In the second, practicing for five minutes on four separate occasions over two weeks had a significantly greater positive effect on self-reported stress than practicing for twenty minutes on four occasions (with nonsignificant trends in the same direction for depression and anxiety).[13] These studies noted the short total program length and the relatively small difference between session durations as limitations. The small sample sizes of these studies (n1 = 77, n2 = 71) also indicate they were powered to detect medium or larger effects, which may not be sufficient to detect marginal differences between dose-based conditions. A third study compared daily practice of ten or thirty minutes of either a sitting or movement meditation for two weeks, finding reductions in psychological distress. Though again, despite a greater variation in doses and larger sample size (n3 = 161, albeit still only powered to detect medium effects), no dose-response (nor practice) effects were observed.[14] A fourth study, which compared single mindfulness sessions of ten and twenty minutes, found no difference in outcomes between the two dose conditions for self-reported mindfulness and psychological outcomes.[15] In a further study where session frequency was experimentally manipulated, no statistically significant difference was found between participants practicing twenty minutes per day for two weeks in one “massed” (twenty-minute) session versus two “distributed” (ten-minute) sessions (n4 = 351).[16]
Dose-response effects have also been assessed in MBPs—the most widely adopted, rigorously tested, and empirically supported of all contemporary meditation types.[17] Although studies that experimentally manipulate session duration or frequency are lacking, metaregression modeling of MBPs has been used, with mixed results. While dose in such analyses has been defined in several ways,[18] here we focus only on the home practice element, as it is an integral component of MBPs; participants are encouraged to sustain home practice upon program completion.[19] A meta-analysis of forty-three studies of exclusively mindfulness-based stress reduction and mindfulness-based cognitive therapy (MBCT) by C. E. Parsons and colleagues found a small but significant association between self-reported frequency and length of home practice sessions and combined mental health outcomes, which included anxiety, depression, and stress (r = 0.26, 95 percent confidence interval [CI] 0.19 to 0.34—i.e., a small-to-medium effect).[20] A metaregression of 203 studies that included a broader range of MBPs (including lower-dose programs) by Sarah Strohmaier found no statistically significant dose-response effects on these same outcomes for either recommended or actual practice (including in-session and home practices and exercises), nor the frequency and length of practices.[21] However, caution needs to be employed when comparing the above, since Strohmaier examined study-level variables (dose) and Parsons and colleagues examined participant-level variables.
Dose-response effects in MBPs are still lacking even when dose has been defined in more diverse ways. Metaregression models using different operationalizations of dose (e.g., number of face-to-face sessions, program length, program intensity, and facilitator contact hours) showed no statistically significant dose-response effects on psychological distress outcomes.[22] Similarly, in analyzing data from a popular mindfulness app where dose was operationalized as minutes of use, days of use, and number and type of activities completed, and with different modeling techniques employed, most models failed to detect dose-response effects for psychological distress.[23] In a randomized controlled trial where program length for an online MBP was experimentally manipulated, there was no statistically significant difference in outcomes between an eight-week program with weekly twenty-minute sessions and a shorter three-week program with weekly twenty-minute sessions.[24]
As highlighted above, the lack of a dose-response relationship observed in most studies and analyses does not imply the absence of such an effect. Notably, most studies have been constrained by the narrow range of session-length dose variations based on conventions developed from previous programs and research evaluations. Experimental studies to date have only compared two session-length dose variations, while most programs in the aforementioned reviews featured recommended formal home practice of thirty to forty-five minutes daily.[25] And since meta-analyses do not experimentally manipulate dose, causation of the effects of different doses cannot be inferred. Further, given such analyses are conducted on effect sizes from overall program content that features multiple active and mutually reinforcing elements (including but not limited to the social aspects inherent in groups, group-based practice, and home-based practice), it is not known to what extent variation in home practice time itself contributes to overall outcomes.[26] Moreover, estimates indicate that an average of fourteen to twenty-two hours could be attained in home practice (assuming thirty to forty-five minutes, six days a week, over eight weeks, with approximately 60 percent adherence).[27] However, an average of seven to fourteen hours of practice would be attained solely within the group context (assuming 50 percent to 100 percent of sessions are completed), thus creating a minimum amount of practice and a restricted dose range. In sum, some existing meta-analysis models critically rely on the limited and relatively low variation in session-length doses (i.e., variability in home practice over and above the minimum of group practice) and hence may be ill-equipped to inform optimal dose guidelines.
Reviews have also highlighted the recent proliferation of single-session “mindfulness inductions” of ten minutes or less.[28] Despite their pragmatic appeal, such low-dose interventions have only demonstrated limited, mixed evidence of effects across a range of transient state-based and (to a lesser extent) dispositional trait-based psychological outcomes.[29] We acknowledge that improvements in psychological “states” could improve wellbeing and promote positive behaviors, and may form the basis of more stable “trait” changes.[30] Further, mindfulness inductions may provide information about the mechanisms engaged at the earliest stages of training, notably including placebo and common factors effects.[31] It is questionable, though, whether mindfulness inductions contribute to the question of dose-response effects, given the one-off nature of such training. Original Buddhist perspectives emphasize the gradual acquisition of mindfulness and related capacities by employing systematic training over time, including rest periods.[32] This process may be analogous to skill acquisition and learning processes more generally, which are predicated on the importance of repeated practice and time for consolidation.[33] Therefore, while studies investigating mindfulness inductions may provide useful information on state-based measures or mechanisms of change, they may be ill-equipped to inform the empirical question of what minimum dose is required for lasting practice effects.
At the other end of the spectrum are studies in high-dose settings like residential meditation retreats,[34] which may be an important avenue for consolidating practice effects and transmitting knowledge in more traditional contexts. Empirical evidence suggests that retreats may confer real and enduring benefits in some individuals, as evidenced by exceptional traits in several psychological, cognitive, and neurological domains.[35] Due to the lack of randomization, though, results in such studies are likely to suffer from self-selection effects.[36] There is also a lack of understanding about whether retreats are suitable for all practitioners, with some evidence suggesting that adverse events may be more likely to occur in this context.[37]
Several studies have used cumulative practice time over a period of sustained practice to probe dose-response relationships, where variation in practice time arises from natural differences in adherence across participants rather than planned manipulations. While most, though not all, findings support a positive correlation between practice time and outcomes, the potential for bias due to the nonrandom distribution of variation in practice time is an important consideration.[38] That is, it may very well be that those who benefit most from practice are more likely to continue to practice, while those who benefit less or experience undesired effects are more likely to discontinue practice. Over time, such differences may lead to a biased representation of individuals with higher amounts of practice showing more marked benefits (as those who have not experienced such benefits may long since have discontinued practice).
What Are the Origins of Dose Conventions?
Before its adaptation into a modern secular context, a relatively small proportion of monastics and dedicated lay practitioners practiced mindfulness meditation to achieve transcendent soteriological goals.[39] Classical Buddhist texts emphasize these goals by stressing the importance of continuous and effortful mindfulness training. Also emphasized, though, was the benefit of establishing a “middle path” of wise effort to avoid extremes of excessive striving and stagnation,[40] particularly during preliminary stages of practice.[41] Beyond these general guidelines, classical texts tended not to recommend specific amounts of practice but instead served as a guide for teachers providing personalized meditation instructions as part of comprehensive religious training.[42]
Early Asian Secular Buddhist Teachers
The modern mindfulness movement has its direct roots in early twentieth-century Burma, where efforts were made to spread meditation among the laity to preserve Buddhist culture in the face of colonialism.[43] Practice in what came to be known as the Insight/Vipassana tradition had many characteristics of the monastic traditions from which it emerged, with the importance of practice emphasized over worldly pursuits and instructions transmitted in dedicated meditation centers under the personal guidance of a teacher. Recommended practice doses reflected this commitment. Ledi Sayadaw, an important teacher in this movement, recommended one to two hours of formal practice per day during preliminary concentration practices, and three to four hours per day for more advanced “insight” practice.[44] Another important teacher was S. N. Goenka, who established a ten-day residential retreat for lay practitioners in 1969 (which has since spread around the world) in which practitioners effectively live like monastics by practicing ten hours daily and adopting Buddhist-derived ethical precepts. Similarly intense practice regimes were recommended outside the retreat setting, with Goenka recommending two hours of formal practice per day,[45] a similar amount to other influential teachers within this lineage.[46]
Early Western Secular Buddhist Teachers
The widespread adoption of mindfulness meditation in nontraditional settings can largely be traced back to the 1960s and 1970s, when the Insight and Zen traditions captured Western interest.[47] It is in this context that dosage recommendations became more relevant as meditation began competing with other activities and therapeutic modalities that contribute to a fulfilling life. We argue that the current understanding of mindfulness meditation dosage has been shaped by a relatively small number of influential forces in this movement. We conducted a cursory review (described in the appendix) of a noncomprehensive sample of popular mindfulness books and online materials from twenty prominent mindfulness meditation experts aligned with an established practice tradition (many of whom taught during the 1960s and 1970s; see table S1) and found several with explicit dose recommendations relating to both session duration and frequency.
For session frequency, across the included sources, there was a consistent emphasis on the importance of daily or near-daily formal practice (time allocated specifically to meditation practice vs. informal practice—incidental use of meditation-related techniques in daily life). Additionally, several experts advocated practicing twice per day.[48] One notable variation from the recommendation for at-least-daily practice was near-daily practice. Thich Nhat Hanh advocated for a “lazy day,” essentially allowing for a day off from everything (including formal meditation).[49] This approach aligns with behavior change principles that have a slightly more forgiving approach to a misstep or lapse, allowing the individual to be less rigid in implementing a change in habits.[50]
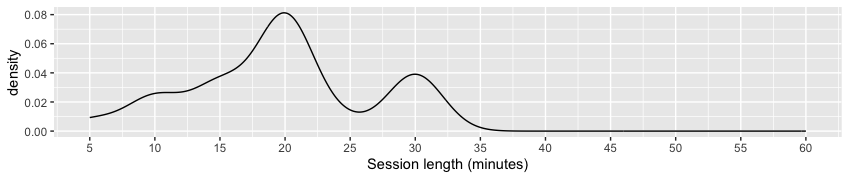
For session duration, most experts recommended that beginners practice for approximately fifteen to thirty minutes per day, working toward forty to sixty minutes over time. Given the consistent emphasis on daily practice, though, several teachers recommended beginners start with as little as five minutes per day to support the establishment of a daily practice habit.[51] There was also some flexibility in recommendations for more experienced practitioners; daily practice of an hour or more was explicitly recommended by some experts.[52] Furthermore, experts commonly recommended supplementing daily practice with periodic extended retreats,[53] which typically include formal practice approximating six to twelve hours per day over one week to several months.[54] The distribution of session durations from this review is presented in figure 1a.

Face-to-Face MBPs
Beyond these Buddhist-influenced views, MBPs also typically recommend that participants engage in formal home practice both during and after the program’s completion.[55] In the original MBSR course, program developer Jon Kabat-Zinn recommended thirty to forty-five minutes of formal daily home practice.[56] This recommendation was based on an “intuition,” which, given Kabat-Zinn’s personal experience practicing within the Insight and Zen traditions, likely had its roots in these practice traditions.[57]
While the MBSR format is still commonly used, a plethora of modified MBPs have been created that vary in certain components, including home practice session duration. Our review of a dataset from a recent meta-analysis on MBPs found 203 randomized controlled trials, with formal practice recommendations documented in 88 percent (n = 183) of included studies.[58] For session duration, the median was 40 minutes, the mean was 35.9 (SD =14.8), and the modal session durations were 45 minutes (30 percent; n = 62) and 30 minutes (20 percent; n = 41). In total, 60 percent of programs retained the original formulation of thirty to forty-five minutes of formal home practice, while just over a quarter of programs (26 percent; n = 54) recommended less than thirty minutes of home practice. Adherence data, however, suggests that participants struggle to complete home practice recommendations, irrespective of session duration. In the 71 percent of studies for which this data was reported, adherence with practice recommendations approximated 58 percent.[59] For session frequency, the vast majority of included MBPs recommended daily (i.e., seven days per week; 71.6 percent, n =131) or near-daily (i.e., six days per week; 22.4 percent, n = 41) practice.
Digital MBPs
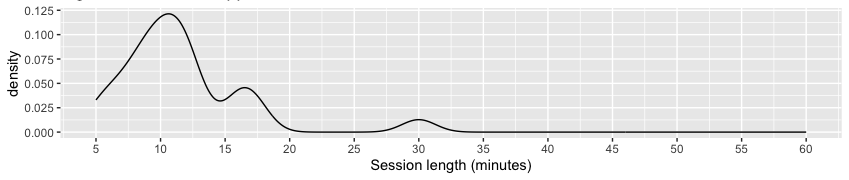
In recent years, MBPs have been increasingly delivered online, and often asynchronously, representing a departure from traditional in-person delivery.[60] While online programs have obvious advantages in terms of access, allowing programs to be delivered at a much greater scale, they also necessitate program adaptations that may have yet unknown consequences.[61] Recent reviews highlight that online MBPs commonly feature shorter practices than more traditional programs. In the Strohmaier meta-analysis database, online and self-help programs included a mean recommended session duration of twenty-six minutes (range six to sixty minutes) compared to thirty-eight minutes (range ten to sixty minutes) for programs delivered in person.[62] The distribution of session durations from this review is shown in figure 1b. There were no differences in practice frequency recommendations in online MBPs relative to face-to-face MBPs.
Mindfulness Apps
The trend toward online programs with shorter practice lengths is even more evident outside MBPs, especially in mindfulness apps.[63] In recent work, over 50 percent of a diverse sample of contemporary meditation practitioners reported using an app to support their practice.[64] Apps may therefore have an increasingly important impact on the way contemporary meditators practice mindfulness, including framing the question of dose via the length of guided practices. For session duration, a recent meta-analysis of thirteen mindfulness apps revealed a range from three to thirty-seven minutes, with a modal value of ten minutes.[65] To further investigate, we cursorily reviewed a noncomprehensive sample of twenty popular mindfulness-specific apps (detailed in the appendix). We found that session duration within programs targeted at relative beginners typically ranged from eight to thirteen minutes (mean = 11.5 minutes), while sessions for ongoing practice were typically slightly longer. The distribution of session durations from this review is shown in figure 1c. While longer practices (i.e., thirty minutes or more) were sometimes offered, they were generally less visible within the app. For session frequency, most apps encouraged daily practice with features such as daily reminders, tracking, and streaks.[66]
Sources of Variation in Dose Recommendations
The above examples highlight that while session frequency is relatively consistent across reviewed sources, session duration is highly heterogeneous. Daily practice frequency was consistently recommended, with experts almost universally emphasizing its importance, and programs (including MBPs and mobile apps) structured to encourage daily practice. While the reasons for daily or near-daily practice were typically not made explicit in the sources we reviewed, mindfulness has often been described as a skill, and therefore similar principles may apply to learning mindfulness as to other kinds of skills (e.g., motor or cognitive) for which the importance of regular practice has been emphasized.[67] While available empirical evidence (though primarily from structured MBPs) is mostly based on daily or near-daily practice, the lack of variation in session frequency has prevented the effects of more and less frequent practice regimes from being tested empirically. More research is needed to determine whether similar benefits are achievable with less frequent practice, or whether greater benefits can be achieved through more frequent (possibly combined with shorter) sessions. K. M. Riordan and colleagues’ recent study is a good first step in this regard.[68]
In contrast to session frequency, there is a large variation in session duration. Among meditation teachers whose materials we reviewed, variation is primarily a function of meditator proficiency, with recommendations approximating fifteen to thirty minutes for beginners and up to forty-five minutes or more for experienced practitioners. Surprisingly, MBSR recommends daily practice toward the upper end of this range, between thirty and forty-five minutes, despite such programs consisting mainly of beginners.[69] The teacher and peer engagement enjoyed by MBSR participants may help to support and motivate their practice at a dosage level that Kabat-Zinn and other experts recommend for ongoing long-term practice while minimizing dropout.[70] With the growing prevalence of online programs, there is some evidence of attenuated session durations in MBPs. And in mindfulness apps, variation in the session duration of guided practices is generally low, with an approximate average of ten minutes.
Insights into Balancing Engagement Versus Efficacy
The potential benefits of longer practice sessions need to be considered alongside potential pitfalls. Longer sessions are theorized to provide several benefits, including allowing more time to develop deeper states of relaxation and concentration,[71] to provide the opportunity to “mindfully” engage with difficult states,[72] to develop more “advanced” stages of meditative insight,[73] and to cultivate more sustained dispositional mindfulness in daily life.[74] However, prior to developing sufficient proficiency, the recommendation to practice more (i.e., via longer practice sessions) may be ineffective or even harmful for some people.[75] Longer sessions can have several inherent challenges, particularly the experience of pain and difficult mental states, which may present a barrier to starting or maintaining a regular mindfulness practice if inadequately addressed.[76] In the small number of dose studies that have been conducted to date, a negative association between session duration and adherence has been observed.[77] Qualitative research around practice in MBPs highlights that time commitment is perceived to be an important reason for nonadherence to recommended practice guidelines.[78]
Shorter sessions may therefore be advantageous for establishing and maintaining a consistent daily practice, which experts almost universally recommend. Positive behavior change, such as the adoption of a daily mindfulness meditation practice, is fostered through several factors including consistent performance of a behavior, the simplicity or complexity of the behavior, and the sense of satisfaction that comes from performing the behavior.[79] Shorter sessions may be easier to incorporate into a daily routine, aiding in habit formation, while skillfully avoiding the challenges of longer sessions.[80] Shorter sessions may also provide a better match between the challenge of maintaining mindfulness during a practice session and a practitioner’s capacity to do so. Relatedly, shorter sessions may be more likely to create positive feelings and a sense of accomplishment and satisfaction that could boost intrinsic motivation for future practice.[81] Following this logic, several experts suggest commencing meditation practice with as little as a few minutes of practice per day, which may explain why meditation apps (predominantly used by novices) prefer low doses.[82] Critically, though, while behavior change principles are known to be effective in other contexts, it is unknown whether low-dose practice—with or without additional behavior change strategies commonly found in apps—support user engagement in the short or long term. Baumel and colleagues estimated that mental health apps retain only 5 percent of users ten days after an app is downloaded, and there are still questions around efficacy even for the 5 percent who do persist.[83] In a recent review of meta-analyses of mental health interventions delivered via mobile apps (18 percent of which were for meditation apps), Simon B. Goldberg and colleagues failed to find convincing evidence of efficacy for any outcome.[84]
Optimal Dose Depends on a Meditator’s Goals, Motivations, and Practice Context
Recommendations to increase session duration over time may also reflect the influence of more traditional practice settings in which the experts in our review were embedded, and the goals inherent to those traditions. Peter Sedlmeier and Jan Theumer identified seventy-one motivations for meditating across thirteen factors, broadly categorized into dealing with problems, managing emotions, exploring or improving aspects of the self, or seeking spiritual experiences.[85] Cross-sectional work suggests that beginner practitioners tend to favor goals associated with mental health and general wellbeing, while more experienced practitioners favor more spiritual goals, indicating that practice goals may change over time.[86] In recent work, the strength of spiritual growth as a practice goal (measured on a scale of 1 to 100) was found to be positively associated with self-assessed daily practice need (r = 0.25, p [p-value] < 0.001), meaning that practitioners who placed a higher value on spiritual growth believed they needed more daily practice than practitioners who valued spiritual growth less.[87] While longer-length sessions and periods of intensive practice may suit practitioners who practice for spiritual growth, it was also found that 40 percent of experienced meditation practitioners (more than five years of active practice) still regarded spiritual growth as a relatively unimportant practice goal.[88] For those practitioners, incremental increases in session durations and periods of intensive practice may be unnecessary above a certain amount if practice goals can be achieved with more modest amounts of practice.
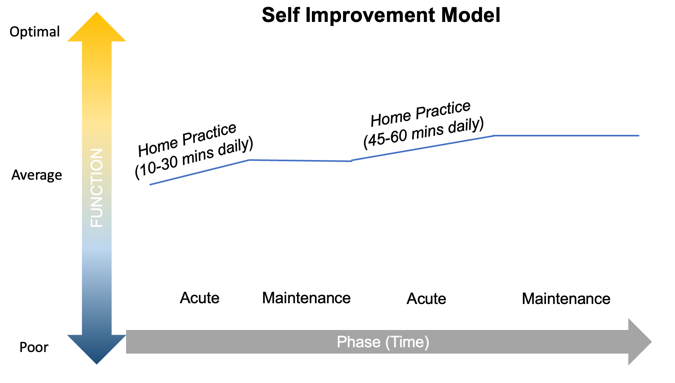
The mode of practice is a further concern when considering the appropriateness of different doses of mindfulness meditation. Above, we have referred to three main contexts within which people practice meditation: self-directed formal home practice, secular MBPs, and residential retreats. Each has different recommended dosage parameters and, by inference, response trajectories. Over time, practice can fit (to varying degrees) within an acute or maintenance phase of practice, where meditative capacities are either developed/enhanced or maintained/consolidated. To capture these dynamics, we have conceptualized three modes of practice: the Clinical Treatment Model, the Self-Improvement Model, and the Spiritual Growth Model (see figure 2).
In the Clinical Treatment Model, the acute practice phase involves practitioners commencing mindfulness meditation to alleviate mental health symptoms by completing a MBP such as MBSR or MBCT. A stated goal of such programs is to optimize wellbeing in the long term, and participants are encouraged to continue engaging in formal practice of thirty to forty-five minutes per day after program completion to consolidate the program’s effects.[89] In the Self-Improvement Model, practitioners engage in self-directed practice to promote wellbeing or manage subclinical mental health symptoms. The acute phase of practice involves developing a daily practice habit with relatively short sessions, increasingly with the support of a mindfulness app or online MBP. Practitioners can choose to continue to practice at this amount or, as the meditation teachers in our review universally recommend, increase practice time (via longer sessions) to promote continued meditative development. In the Spiritual Growth Model, the acute phase of practice is often in the context of a residential retreat, such as in the Insight/Vipassana tradition, where practitioners engage in approximately ten one-hour sessions per day for ten days. Thereafter, participants in one popular tradition are encouraged to practice twice daily for an hour as a way of maintaining the meditative capacities that were developed during the retreat, and to complete subsequent retreats annually.[90] In reality, practitioners may move between these modes of practice as proficiency is developed and goals of practice shift over time, as represented in figure 2.

| 
|

| 
|

|
Although meditation teachers generally extol that “more is better” when it comes to meditation dosage (including progressively longer sessions and periods of intensive practice), there is as yet limited empirical support for a positive dose-response relationship. If a positive relationship is demonstrated, the question remains whether the marginal benefits of longer practices accrue linearly with increases in dose, or whether incremental increases in session duration become subject to diminishing returns. In the related field of psychotherapy, K. I. Howard and colleagues theorized a log-linear relationship between the number of psychotherapy sessions and mental health outcomes.[91] Recent work by our group found support for a similar relationship following meditation practice, with evidence for possible diminishing returns above approximately two hundred hours of cumulative practice hours.[92] However, substantially more empirical evidence is needed to confirm whether similar effects are evident for longer sessions of meditation, and what the optimal amount of meditation may be based on practitioners’ goals, experiences, and capacities, and the context within which they practice (i.e., self-directed formal home practice, secular MBPs, residential retreats, etc.).
Recommendations for the Dose-Response Research Agenda
Dose-response studies to date have suffered from several problems, including the use of a narrow range of doses, short overall program length, the presence of confounding variables due to comparing dose-related effects across programs, and bias from the nonrandom distribution of participants across different doses. These have limited the empirical understanding of dose-response effects for mindfulness meditation. Although our literature search was nonsystematic, the trends identified by this work allow us to propose several avenues for answering the most pressing questions about mindfulness meditation dosage, as described in table 1.
Table 1: Summary of Key Considerations and Proposed Solution for Dose-Response Studies
| Considerations | Problem | Solution |
|---|---|---|
Study attrition | Likelihood of differential rates of attrition across conditions creates bias | Run-in period to minimize post-randomization attrition, and sufficient incentives for participants to continue providing data regardless of intervention adherence |
Outcome measure sensitivity to detect small differences between doses | Claims of equivalency based on lack of significant differences may be an artifact of insufficiently powered studies | Power studies to detect small effects. Multimodal assessment of processes theorized to underlie mechanisms of change in mindfulness interventions (i.e., decentering, equanimity, etc.) |
Study design | Study design and statistical analysis should account for the study’s primary focus: efficacy or effectiveness | Study design should focus on efficacy and encourage adherence Pilot work can be done to ascertain willingness to participate in differential dose allocations. Per-protocol analysis may be better than intention to treat, but reasons for nonadherence need to be actively investigated for safety |
Practitioner experience with meditation | Appropriateness of measures may differ across different levels of practitioner experience | Ensure outcome measures align with practitioner goals and practice motivations |
Intervention length | Very short or low-dose interventions may be ill-equipped to detect stable trait effects | Meditation dosage should be investigated in an intervention of sufficient overall length to produce more stable “trait” effects |
Different dose recommendations may be appropriate for different practitioners | Use of overall means and effect sizes obscures individual-level differences | Power the trial to analyze prespecified subgroups |
At present, the limited body of evidence points toward there being no difference in outcomes between larger and smaller doses. This conclusion conflicts with recommendations from meditation teachers, who theorize a positive dose-response relationship. That is, experts recommend beginners start with relatively short sessions (fifteen to thirty minutes) that increase over time when more experience is gained (with several explicitly noting the benefits of longer sessions). We suggest that future studies experimentally manipulate a broader range of treatment doses in randomized controlled designs in which bias is minimized and the factors determining optimal meditation dosage for different types of individuals can be studied. This way, the conflict between expert recommendation and empirical data can be reconciled, and the field can work toward developing personalized recommendations for session duration and frequency based on empirical evidence that matches the proficiency and capacity of practitioners at different stages of their meditation path. The traditional (i.e., teacher recommendations) and empirical evidence we have reviewed here can inform many aspects of the design of such studies, including the range of doses to be considered (i.e., five to thirty minutes for beginners). Further, we recommend that interventions include a postintervention follow-up to monitor whether different dose-based conditions can predict ongoing practice, the importance of which was commonly emphasized by meditation teachers whose texts we reviewed.
Differences between doses are likely to represent relatively small effect sizes, as such comparisons aim to quantify the difference between two active conditions with the same underlying mechanisms of action, often with subtle differences in practice amounts. To determine whether a longer intervention is more effective than a shorter intervention, we need to consider whether the study is adequately powered (statistically) to detect likely differences. Studies will thus need to be adequately powered and outcome measures sufficiently sensitive to change. Noninferiority designs should also be considered where appropriate. Interventions should also be of sufficient overall length to detect more stable trait effects, which mindfulness induction studies may fail to produce. As a start, we recommend interventions of at least four weeks to align with the most common length of intervention that has been tested for meditation apps and the mean length of app-based programs included in our review.[93] Failing these measures, lack of a significant difference should not be confused with evidence of equivalence across doses.
It would be beneficial to focus on multimodal assessment (i.e., behavioral and self-report) of processes theorized to underlie the mechanisms of change in mindfulness, such as attention regulation, equanimity, decentering, and emotion regulation.[94] It may also be relevant to assess dose-response effects independently across different outcome measures, as the resulting dose-response curves may differ in important ways. Bayesian analyses may provide valuable insights into dose effects and dynamics, as such analyses have the advantage of incorporating prior information based on the available data to estimate the likelihood that hypothesized differences between doses are supported.
A further key challenge for dose-response studies will be their design and implementation to minimize bias associated with differential rates of attrition. Study attrition is a key challenge in psychological research generally, especially research on mental health apps.[95] It may be particularly relevant to dose-response studies, though, given the likelihood of higher rates of attrition for longer doses.[96] To minimize bias, study participants should be encouraged and incentivized to continue honestly reporting their practice amount and responding to questionnaires regardless of whether they are still undertaking the intervention. Significant effort will be required to get true estimates of adherence to the intervention while also minimizing study-related attrition. The latter may benefit from using a “run in” period prior to commencement of the actual trial, consisting of asking participants to complete surveys each day, so that those participants who are most likely to drop out of the study do so before randomization. Such designs, however, will not capture true engagement rates as sizeable proportions of the initial sample may quit early.[97]
Although dose-finding studies need to first understand what effects different doses have under ideal conditions where practitioners practice as intended (i.e., efficacy), they also need to consider whether such doses are feasible in real-life scenarios. In the evidence we reviewed, the recommendation for beginners to start with relatively short sessions was largely due to perceived challenges of longer sessions and the difficulties of maintaining a meditation routine in the early stages of practice.[98] However, the recommendation to increase session duration over time was motivated by perceived benefits of longer sessions. This suggests a tension between engagement (and hence effectiveness) and efficacy that can be tested empirically in well-designed dose-finding studies.
For questions of efficacy, a per-protocol design may be optimal. It would be important, though, for as many participants as possible to adhere to dose recommendations to avoid differential nonadherence having an impact on outcomes. Advanced statistical approaches may be able to help adjust for differential nonadherence.[99]
To understand engagement, survey and pilot studies can ascertain willingness to participate in differential dose allocations. It is crucial to distinguish between study attrition and intervention adherence, and to measure both independently, so we know what happens to those whose adherence to the intervention is low. With the move toward digital interventions, the availability of objective user data is likely to also provide a level of insight into patterns of engagement and use that were not possible via homework practice diaries.
Given that efficacy and engagement may impact one another, it is worthwhile to study these separately to eventually ascertain the minimally effective dose that people are willing to do. Once efficacy and engagement are understood, trials can begin to test the real-life effectiveness of different doses. For this, trials will need to follow the intention-to-treat principle, wherein large samples are necessary, as are adjustments for potential statistical issues.[100] Large-scale studies of apps may help to ascertain the effectiveness of specific programs in real-world settings. Importantly, different study designs may be suited to different contexts when informing the question of optimal dose. For example, a highly motivated and conscientious individual wanting to ascertain the optimal practice dose would be more interested in efficacy trials from per-protocol designs rather than effectiveness trials measuring intention-to-treat effects, where outcomes related to different doses may be impacted by adherence.
Finally, it is important to consider the practice context and potential for individual differences when planning and conducting dose-response studies. The immediate practice context (e.g., self-directed home practice, MBP, or residential retreat) and a practitioner’s experience (and resulting meditative capacities) will likely impact dosage recommendations, as indicated in figure 2. Several other factors specific to the practitioner may also be important, including goals, personality, and mental health status. Prespecified subgroup analyses in sufficiently powered studies can help ascertain whether and how such factors may impact dosage recommendations. In the broader social context, it is crucial to acknowledge that meditation practice is socially and culturally embedded,[101] so the same doses may produce different outcomes in different settings, populations, and cultures. Ignoring these differences can lead to an oversimplification and misrepresentation of the outcomes of meditation practice. At a minimum, settings and contexts of the studies need to be described in detail in the resulting reports, and generalizability claims need to be carefully justified.
Conclusion
Mindfulness meditation has been practiced for millennia across various contexts, over which time it has undergone multiple adaptations. These practices are now increasingly used in secular contexts, where instructions are often delivered on a one-to-many basis and practitioners engage in relatively self-directed and autonomous practice. To support such practitioners, it is essential that we better understand the relationship between dose and outcomes. This will enable the development of guidelines that can inform practitioners and their advisers about the optimal practice dose needed to achieve certain goals. To date, dosing conventions have largely developed from recommendations of popular mindfulness teachers and then have been shaped by the novel contexts that have transmitted mindfulness practices, namely MBPs and mobile applications. While these ready-made formats have provided suitable templates for studying the effectiveness of mindfulness meditation, they have not been optimized for investigating dose-response effects. Rather than relying on the conventions that have developed so far, there is a critical need to underpin dosage recommendations with empirical evidence from well-designed dose-response studies that minimize bias by adopting some of the measures detailed in our dose-response research agenda.
Appendix
S1. Data Behind the Origins of Dose Conventions
Secular Buddhist Sources
We searched books and online sources for meditation dose recommendations from mindfulness teachers who have been influential in the modern mindfulness movement[102] and have taught within a recognized Buddhist practice tradition. Our focus was on materials aimed at relatively novice practitioners that provided guidance on meditation practice dose, particularly regarding session duration. Our main findings are summarized in table S1, while the contexts from which these recommendations were extracted are provided in S2.
Mindfulness Apps
The twenty mindfulness apps included in our review were those available in both Google Play and Apple’s App Store and had at least one thousand reviews in both stores or at least ten thousand reviews in either store. Included apps are listed in the Data_SI data file,[103] which includes the number of reviews in both stores (as of October 2022), the number of days in the selected program, and the mean session duration within that program. Programs were selected if they were featured prominently within the app and were aimed at novice practitioners. In those programs where different dose variants are offered for the same guided practice, a low and high estimate has been included. For the Insight Timer app, various programs are offered, and so we calculated the mean session duration for twenty prominent programs, all of which have at least twenty thousand reviews. The low and high value for the Insight Timer app represents the 10th and 90th percentile of the average session duration across the twenty programs.
Mindfulness-Based Programs
Data extracted from the Strohmaier meta-analysis pertaining to recommended session duration and frequency for home practice is reproduced in the Data_SI file.[104]
Table S1: Dose Recommendations from Traditional Sources | ||||||
# | Teacher | Tradition / context | Began teaching | Practice duration based on proficiency | ||
Novice | Intermediate | Advanced | ||||
1 | Brach, T. | Psychologist and teacher within the Insight/Vipassana practice tradition | ~1998 | 15 mins | – | 45 mins |
2 | Chödrön, P. | Teacher and monastic within the Kagyü Buddhist tradition | ~1980 | 20 mins | 40 mins | 1 hour |
3 | Feldman, C. | Teacher within the Insight/ Vipassana practice tradition | 1976 | 15–30 mins | – | – |
4 | Goldstein, J. | Teacher within the Insight/Vipassana practice tradition | 1974 | 20–30 mins | Gradually extend by 10–15 mins | No upper limit |
5 | Hanh, T. N. | Teacher and monastic within (and founder of) the Plum Village tradition | 1975 | 20–30 mins | – | – |
6 | Kabat-Zinn, J. | Founder of mindfulness-based stress reduction program | 1979 | – | – | – |
7 | Kornfield, J. | Teacher within the Insight/Vipassana tradition | 1975 | 15 mins | 30 mins | 1+ hour |
8 | Mahathera, H. Gunaratana | Teacher and monastic within the Insight/Vipassana tradition | 1968 | 20 mins | 5 mins more than comfortable | 1 hour |
9 | McDonald, K. | Teacher and monastic within the Tibetan Buddhist tradition | 1974 | 10–30 mins | – | 1+ hour |
10 | Mingyur, Y. | Meditation master within the Karma Kagyü and Nyingma lineages of Tibetan Buddhism | – | 20 mins | – | – |
11 | Rāhula, W. | Mahasi Sayadaw Vipassana lineage of Theravada Buddhism | – | 5–10 mins twice daily | “Longer and longer periods” | |
12 | Ricard, M. | Teacher and monastic within the Tibetan Vajrayana tradition | – | 20 min | – | |
13 | Rosenberg, L. | Teacher within the Insight/Vipassana tradition | 1985 | 15–20 mins | 45–60 mins | |
14 | Salzberg, S. | Teacher within the Insight/Vipassana tradition | 1974 | 20 mins | 30–45 mins | |
15 | Sumedho, A. | Teacher and monastic within the Insight/Vipassana tradition | ~1980 | 10–15 mins | – | – |
16 | Titmuss, C. | Teacher within the Insight/Vipassana practice tradition | – | 20 mins | 40 mins twice per day | |
17 | Trungpa, C. | Kagyü Buddhist lineage of Tibetan Buddhism | 1970 | 15 mins | – | 1 hour |
18 | Wallace, B. A. | Teacher within Tibetan Buddhism | 1975 | 24 mins | 48 mins | “Many hours per day” |
19 | Winston, D. | Teacher within the Insight/Vipassana tradition | 1999 | 5 mins | – | 20–30 mins |
20 | Yates, J. (Culadasa) | Teacher and monastic within the Insight/Vipassana tradition | ~1980 | 15–20 mins | 45 mins | > 45 mins |
Mean | 20 mins | |||||
Notes. For mean calculation, when a range was provided the midpoint was used. For the context within which these recommendations were made, see S2. | ||||||
S2. Excerpts from Sources of Dosage Recommendations
1. “How long should I sit each day? Deciding in advance the duration of your sit can help support your practice. For many, a good time frame is between 15–45 minutes. If you sit each day, you’ll gradually experience noticeable benefits (e.g., less reactivity, more calm) and be more inclined to increase your sitting time. If you’re just beginning a meditation practice, you might want to experiment with the length of time that you meditate. You might choose to meditate for just five minutes once or twice a day, and increase the time by five minutes a day until you reach a length of time that you can commit to on a daily basis.”[105] (Tara Brach)
2. “Next, consider how long you will practice. How long will you sit for? You can sit for twenty minutes or two hours; this is up to you. But set yourself up for success. When you commit to a meditation practice, you don’t want to put yourself in a position where you will easily feel defeated. For beginning meditators, I suggest starting with twenty minutes. Then after a month or several months of practice, you can lengthen your time by another twenty minutes. If you are a seasoned meditator or if you are returning to a meditation practice, you might commit to an hour a day.”[106] (Pema Chödrön)
3. “It is helpful to create a time in our day that is regularly dedicated to our formal meditation. When we wake in the morning or before going to bed at night are times that lend themselves well to a period of stillness and reflection. Making these periods of meditation into a reliable part of our daily routine is an invaluable asset in developing a path of practice. We may begin with fifteen-minute or half-hour periods. It is all worthwhile. It is helpful to approach these times with great care—they are not times for rehearsing our day or pondering upon what has been left undone. They are times for focus and dedication.”[107] (Christine Feldman)
4. “To start with I think it’s good to set an amount of time that you feel workable, that inspires you to do it, that is not going to feel too daunting. So people could choose almost any amount of time. It can be twenty minutes or half an hour. The important thing is the regularity of it. Pick an amount of time that you really feel committed to doing every day. It’s the everyday-ness that is going to build the practice. Over time people may find that they get comfortable with that amount of time and they may feel, ‘What it would be like to extend it for 10 or 15 minutes?’ So there is no absolute number that we need to work with. I think it’s starting with what feels doable and actually inspires one to do it and then gradually expand the time as one feels necessary. At a certain point, for people who have developed a strong practice sitting an hour a day would be great. Some people sit 2 hours a day, so there is no upper limit.”[108] (Joseph Goldstein)
5. “For beginners, it is better to sit no longer than 20 or 30 minutes. During that time, you can readily obtain total rest. The technique for obtaining this rest lies in two things—watching and letting go: watching your breath, and letting go of everything else. Release every muscle in your body. After about 15 minutes or so, it is possible to reach a deep quiet filled with inner peace and joy. Maintain this quiet and peace. Some people look on meditation as a toil and want the time to pass quickly in order to rest afterwards. Such persons do not know how to sit yet. If you sit correctly, it is possible to find total relaxation and peace right in the position of sitting. Often it helps to meditate on the image of a pebble thrown into a river.”[109] (Thich Nhat Hanh)
6. “How long a period of time should you start with? There’s no real prescription but I would say it’s good to try 15 minutes: long enough so that you get really bored and antsy and learn how to make room for unpleasant moments. You have to have it be long enough so that you experience a lot of different body and mind states like the discomfort from being still. Then that becomes your teacher instead it being bad or an impediment to being mindful. You notice any thoughts, like ‘I hate this,’ ‘It’s boring and stupid’ and then recognize that these are just thoughts. You may have lot of emotions like impatience and frustration and think, ‘Well I just can’t meditate’ and perhaps you get down on yourself or decide to throw in the towel. But the whole point is to just simply notice the play of the mind and body, and not taking things personally when they aren’t.”[110] (Jon Kabat-Zinn)
7. “It keeps coming up, this question of how long to meditate. We felt from the beginning of our work using meditation with patients in the hospital that it would be important for them to be exposed right from the start to relatively extended periods of practice. Since we believed strongly in the principle that if you ask a lot of people or ask them to ask a lot of themselves, then you will get a lot, whereas if you ask only a little, the most you are likely to get is a little, we went with forty-five minutes as the basic required practice time at home every day. Forty-five minutes seemed long enough to settle into stillness and sustained attending from moment to moment, and perhaps to experience at least tastes of a deepening relaxation and sense of well-being. It also seemed long enough to allow for ample opportunity to engage the more challenging mind states that we ordinarily hope to avoid because they take over our lives and severely tax (when they don’t overwhelm completely) our ability to remain calm and mindful. The usual suspects, of course, are boredom, impatience, frustration, fear, anxiety (which would include worrying about all the things you might be accomplishing if you weren’t wasting time meditating), fantasy, memories, anger, pain, fatigue, and grief. It turned out to be a good intuition. Most of the people coming through our clinic have willingly made the almost never easy adjustments in the day-to-day conduct of their lives to practice daily for forty-five minutes at a stretch, at least over a period of eight weeks. And many never stray from that new life path. It not only becomes easy, it becomes necessary, a lifeline.”[111] (Jon Kabat-Zinn)
8. “Select a regular time for practice that suits your schedule and temperament. If you are a morning person, experiment with a sitting before breakfast. If evening fits your temperament or schedule better, try that first. Begin with sitting ten or twenty minutes at a time. Later you can sit longer or more frequently. Daily meditation can become like bathing or toothbrushing. It can bring a regular cleansing and calming to your heart and mind.”[112] (Jack Kornfield)
9. “A similar rule applies here: sit as long as you can, but don’t overdo it. Most beginners start with twenty or thirty minutes. Initially, it’s difficult to sit longer than that with profit. The posture is unfamiliar to Westerners, and it takes a bit of time for the body to adjust. The mental skills are equally unfamiliar, and that adjustment takes time, too. As you grow accustomed to the procedure, you can extend your meditation little by little. We recommend that after a year or so of steady practice you should be sitting comfortably for an hour at a time. Here is an important point, though: vipassana meditation is not a form of asceticism. Self-mortification is not the goal. We are trying to cultivate mindfulness, not pain. Some pain is inevitable, especially in the legs. We will thoroughly cover pain, and how to handle it, in chapter 10. There are special techniques and attitudes that you will learn for dealing with discomfort. The point to be made here is this: This is not a grim endurance contest. You don’t need to prove anything to anybody. So don’t force yourself to sit with excruciating pain just to be able to say that you sat for an hour. That is a useless exercise in ego. And don’t overdo it in the beginning. Know your limitations, and don’t condemn yourself for not being able to sit forever, like a rock. As meditation becomes more and more a part of your life, you can extend your sessions beyond an hour. As a general rule, just determine what is a comfortable length of time for you at this point in your life. Then sit five minutes longer than that. There is no hard and fast rule about length of time for sitting. Even if you have established a firm minimum, there may be days when it is physically impossible for you to sit that long. That doesn’t mean that you should just cancel the whole idea for that day. It’s crucial to sit regularly. Even ten minutes of meditation can be very beneficial.”[113] (H. Gunaratana Mahathera)
10. “In the beginning it is best to meditate for short periods—ten to thirty minutes—and end your session while mind and body are still comfortable and fresh. If you push yourself to meditate for too long and rise from your seat with an aching body and a frustrated mind, you won’t have much interest in sitting down to meditate again. Meditation should be a satisfying and productive experience, not a burden.
“Meditate for short periods—ten to thirty minutes—until your concentration has improved. Then you can sit for an hour or more, or as long as you can maintain strong awareness. If the meditation is going well, you will feel light and relaxed.”[114] (Kathleen McDonald)
11. “Is it important to have a daily meditation practice?”
“The ultimate goal of meditation practice is to bring awareness to every moment of one’s life, not just the time one spends in a formal meditation session. That said, setting aside time each day to cultivate awareness is an indispensable part of the process. Most people find that the more time they devote to meditation ‘on the cushion,’ the easier it is to bring awareness to their experiences ‘off the cushion.’”
“How long should I meditate?”
“When beginning a daily meditation practice, it is important to meditate in short, frequent sessions. Twenty minutes a day, practiced over one or two sessions, is a good general guideline for beginning meditators. It is important to note, however, that you can and should practice anytime, anywhere. Once you know the key points of meditation, you will be able to use any experience or activity as a way to practice sustaining meditative awareness.”[115] (Yongey Mingyur Rinpoche)
12. “You breathe in and out all day and night, but you are never mindful of it, you never for a second concentrate your mind on it. Now you are going to do just this. Breathe in and out as usual, without any effort or strain. Now, bring your mind to concentrate on your breathing-in and breathing-out; let your mind watch and observe your breathing in and out; let your mind be aware and vigilant of your breathing in and out. When you breathe, you sometimes take deep breaths, sometimes not. This does not matter at all. Breathe normally and naturally. The only thing is that when you take deep breaths you should be aware that they are deep breaths, and so on. In other words, your mind should be so fully concentrated on your breathing that you are aware of its movements and changes. Forget all other things, your surroundings, your environment; do not raise your eyes and look at anything. Try to do this for five or ten minutes. At the beginning you will find it extremely difficult to bring your mind to concentrate on your breathing. You will be astonished how your mind runs away. It does not stay. You begin to think of various things. You hear sounds outside. Your mind is disturbed and distracted. You may be dismayed and disappointed. But if you continue to practise this exercise twice daily, morning and evening, for about five or ten minutes at a time, you will gradually, by and by, begin to concentrate your mind on your breathing. After a certain period, you will experience just that split second when your mind is fully concentrated on your breathing, when you will not hear even sounds nearby, when no external world exists for you. This slight moment is such a tremendous experience for you, full of joy, happiness and tranquillity, that you would like to continue it. But still you cannot. Yet if you go on practising this regularly, you may repeat the experience again and again for longer and longer periods. That is the moment when you lose yourself completely in your mindfulness of breathing. As long as you are conscious of yourself you can never concentrate on anything.”[116] (Walpola Rāhula)
13. “If we consider that the possible benefit of meditation is to have a new experience of the world each moment of our lives, then it doesn’t seem excessive to spend at least twenty minutes a day getting to know our mind better and training it towards this kind of openness. The fruition of meditation could be described as an optimal way of being, or again, as genuine happiness. This true and lasting happiness is a profound sense of having realized to the utmost the potential we have within us for wisdom and accomplishment. Working towards this kind of fulfilment is an adventure worth embarking on.” [117] (Mattieu Ricard)
14. “At the end of every retreat, I always try to give the new people a few tips for taking the practice back home. It is best to sit every day and to have a place in your house or apartment that is quiet and removed from activity that you can reliably use for that purpose. I can’t really say how long your sitting periods should be. When I teach beginners, I start with periods of fifteen to twenty minutes and gradually work up to forty-five minutes and more. On retreats, sittings run between thirty and sixty minutes—most are forty-five—and the regular sittings that we have here in Cambridge last for an hour. The amount of time is less important than the regularity. It is good to sit a little longer than you want to so you see the part of your mind that resists practice, but you don’t want to torture yourself. In the same way, it is important to sit even on days when you don’t feel like it. If you sit only when you want to, you will know only the mind that likes to sit.”[118] (Larry Rosenberg)
15. “Sit comfortably, with your back erect. It is fine to sit in a chair or on an arrangement of cushions on the floor. If necessary, you can lie down. Close your eyes and take a few deep breaths, feeling the breath as it enters your nostrils and fills your chest and abdomen; then release it. Allow the breath to become natural, without forcing it or controlling it. Let your attention rest on one breath at a time. If your mind wanders, don’t be concerned. Notice whatever has captured your attention, then let go of the thought or feeling, and return to the awareness of the breath. In this way, meditation teaches us gentleness and an ability to forgive our mistakes in life and to go on. I recommend sitting for a 20-minute session if you are just getting started and increasing the time gradually until you are meditating for 30 or 45 minutes. At the end of your meditation period, lovingly acknowledge others in your life—your family or your community, maybe the whole planet. This forms the bridge between our inner work and our resolve to act with more awareness and love in our daily lives. Increase as you become more familiar with the practice. Instructions from a mindfulness teacher or CD will help guide you in starting your practice.”[119] (Sharon Salzberg)
16. “With ānāpānasati, you recognise the way it is now and you start from there: you sustain your attention a little longer and you begin to understand what concentration is, making resolutions that you can keep. Don’t make Superman resolutions when you’re not Superman. Do ānāpānasati, for ten or fifteen minutes rather than thinking you can do it the whole night, ‘I’m going to do ānāpānasati from now until dawn.’ Then you fail and become angry. You set periods that you know you can do. Experiment, work with the mind until you understand how to put forth effort, how to relax.[120] (Ajahn Sumedho)
17. “Sit in a meditative posture once or twice a day, or at least three times a week, for a minimum of twenty minutes per session.”[121] (Christopher Titmuss)
18. “The length of your meditation session may vary from day to day, and the length of time may have a lot to do with family and work obligations. If you can only set aside ten or fifteen minutes a day to sit, start with that. You may find that you can set aside more time on the weekends or when you have time off of work. Although the amount of time you sit from day to day may vary, before you start your session each day, it’s important to decide how long you’re going to sit, and keep to that. If you don’t give yourself a set goal, you might give up after five minutes. So decide before you start how long you’re going to sit. If you have a meditation instructor, you can also discuss your daily sitting practice with him or her, and come up with a plan to increase the amount you practice each week. Or if you don’t have an instructor, you can make your own plan to start with fifteen minutes a day and work up to an hour.”[122] (Chogyam Trungpa)
19. “At the beginning of this training, meditators are traditionally encouraged to practice for sessions of twenty-four minutes, which is one-sixtieth of a full day and night. At the culmination of this training, you should be able to sustain attention with unprecedented clarity for ten times that long.
“When you reach the third stage, resurgent attention, during each practice session your attention is fixed most of the time upon your meditative object. By now, you will have increased the duration of each session beyond the initial twenty-four minutes to perhaps twice that. As your attention gradually stabilizes, you may increase the duration of each session by increments of three minutes. At all times, though, value the quality of your meditation over the quantity of time spent in each session. If you sit for long periods but let your mind rove around unnoticed among distractions or fall into dullness, not only are you wasting your time, but also you are developing bad habits that will only get harder and harder to break.
“Most people would find their lives greatly enhanced just by attaining stage two of the ten stages. This level of development takes some effort, but it can be achieved by people who are living a busy life with career and family commitments as long as they are willing to set aside some time for meditation. It can dramatically improve the quality of everything you do and make you more resilient in the face of emotional and physical stressors. If that is your goal, there is no problem with using the techniques in this book for that purpose. However, as noted above, this book is also a guide for people who wish to go well beyond what are considered normal levels of attention. For most people, achieving stage three will require a greater commitment than an hour or two spent each day in meditation in the midst of an active life. The more advanced stages of attentional development are accessible to people who dedicate themselves to weeks or months of rigorous practice in a conducive environment. Progress beyond the fourth attentional stage requires a vocational commitment to this training, which may involve full-time practice for months or years at a stretch.”[123] (B. Alan Wallace)
20. “The amount of time can vary. I generally start students with just five minutes and work them up to twenty to thirty minutes. I’d rather you start with a short, doable stretch than have you attempt a longer stretch right away and then get discouraged when you can’t sustain it.”[124] (Diana Winston)
21. “Begin with shorter meditations. I suggest fifteen or twenty minutes each day for the first week or two. Then, increase the length of your sessions in five-minute increments weekly or every few days until you reach 45 minutes. Use a meditation timer rather than looking at a clock, and train yourself not to look at the timer. Just listen for the bell. Some people find it easier to do two shorter meditations of 20 to 30 minutes each day. This is fine at first, but I strongly recommend at least one daily 45-minute sit as a minimum. This will provide a solid basis for your practice. As you advance through the Stages and gain more skill, your meditations will become more interesting and enjoyable. You will eventually have no problem extending 45 minutes into an hour and practicing more than once a day if you choose. It’s always best to work up gradually rather than do too much at first and become discouraged.”[125] (John Yates [Culadasa])
Notes
* We have no known conflicts of interest to disclose. The present work was funded via the Contemplative Studies Centre, established by a philanthropic gift from the Three Springs Foundation, Pty. Ltd. Correspondence concerning this article should be addressed to Nicholas Bowles, Contemplative Studies Centre, University of Melbourne, Australia. Email: nbowles@student.unimelb.edu.au. ↑
- J. N. Davies et al., “Prevalence and 20-Year Trends in Meditation, Yoga, Guided Imagery and Progressive Relaxation Use Among US Adults from 2002 to 2022,” Scientific Reports 14, no. 1 (2024): 14987. ↑
- O. Simonsson, S. Fisher, and M. Martin, “Awareness and Experience of Mindfulness in Britain,” Sociological Research Online 26, no. 4 (2021): 833–852. ↑
- D. L. McMahan, The Making of Buddhist Modernism (Oxford University Press, 2008); N. T. van Dam et al., “Mind the Hype: A Critical Evaluation and Prescriptive Agenda for Research on Mindfulness and Meditation,” Perspectives on Psychological Science 13, no. 1 (2018): 36–61. ↑
- See R. S. Crane et al., “What Defines Mindfulness-Based Programs? The Warp and the Weft,” Psychological Medicine 47, no. 6 (2017): 990–999. ↑
- J. Kabat-Zinn, “Some Reflections on the Origins of MBSR, Skillful Means, and the Trouble with Maps,” Contemporary Buddhism 12, no. 1 (2011): 281–306. ↑
- See, e.g., É. Gál, S. Ștefan, and I. A. Cristea, “The Efficacy of Mindfulness Meditation Apps in Enhancing Users’ Well-Being and Mental Health Related Outcomes: A Meta-Analysis of Randomized Controlled Trials,” Journal of Affective Disorders 279 (2021): 131–142; M. Sommers-Spijkerman et al., “New Evidence in the Booming Field of Online Mindfulness: An Updated Meta-Analysis of Randomized Controlled Trials,” JMIR Mental Health 8, no. 7 (2021): e28168. ↑
- J. Galante et al., “Mindfulness-Based Programmes for Mental Health Promotion in Adults in Nonclinical Settings: A Systematic Review and Meta-Analysis of Randomised Controlled Trials,” PLoS Medicine 18, no. 1 (2021): e1003481. ↑
- S. B. Goldberg et al., “Mobile Phone-Based Interventions for Mental Health: A Systematic Meta-Review of 14 Meta-Analyses of Randomized Controlled Trials,” PLOS Digital Health 1, no. 1 (2022): e0000002. ↑
- A. Baumel et al., “Objective User Engagement with Mental Health Apps: Systematic Search and Panel-Based Usage Analysis,” Journal of Medical Internet Research 21, no. 9 (2019): e14567. ↑
- See, e.g., L. G. Sylvia et al., Comparing Standard and Short Online Mindfulness Therapy Programs for Improving Well-Being—The Healthy Mind Healthy You Study (Patient-Centered Outcomes Research Institute [PCORI], 2022). ↑
- C. R. Berghoff et al., “Mindfulness Meditation Adherence in a College Sample: Comparison of a 10-Min versus 20-Min 2-Week Daily Practice,” Mindfulness 8, no. 6 (2017): 1513–1521. ↑
- S. Strohmaier et al., “Effects of Length of Mindfulness Practice on Mindfulness, Depression, Anxiety, and Stress: A Randomized Controlled Experiment,” Mindfulness 12 (2021): 198–214. ↑
- G. W. Fincham, K. Mavor, and B. Dritschel, “Effects of Mindfulness Meditation Duration and Type on Well-Being: An Online Dose-Ranging Randomized Controlled Trial,” Mindfulness 14 (2023): 1171–1182. ↑
- R. Palmer et al., “The Effect of Ten versus Twenty Minutes of Mindfulness Meditation on State Mindfulness and Affect,” Scientific Reports 13, no. 1 (2023): 20646. ↑
- K. M. Riordan et al., “How Often Should I Meditate? A Randomized Trial Examining the Role of Meditation Frequency When Total Amount of Meditation Is Held Constant,” Journal of Counseling Psychology 71, no. 2 (2024): 104–114. ↑
- See Crane et al., “What Defines Mindfulness-Based Programs?” ↑
- S. Strohmaier, “The Relationship Between Doses of Mindfulness-Based Programs and Depression, Anxiety, Stress, and Mindfulness: A Dose-Response Meta-Regression of Randomized Controlled Trials,” Mindfulness 11 (2020): 1315–1335. ↑
- C. E. Parsons et al., “Home Practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A Systematic Review and Meta-Analysis of Participants’ Mindfulness Practice and Its Association with Outcomes,” Behaviour Research and Therapy 95 (2017): 29–41. ↑
- Here, r = a correlation coefficient, which indicates the strength and direction of the linear relationship between two variables. Parsons et al., “Home Practice in Mindfulness-Based Cognitive Therapy.” ↑
- Strohmaier, “Relationship Between Doses.” ↑
- Strohmaier, “Relationship Between Doses.” ↑
- S. B. Goldberg et al., “Is Dosage of a Meditation App Associated with Changes in Psychological Distress? It Depends on How You Ask,” Clinical Psychological Science 13, no. 2 (2024): 332–349. ↑
- Sylvia et al., Comparing Standard and Short. ↑
- Parsons et al., “Home Practice in Mindfulness-Based Cognitive Therapy”; Strohmaier, “Relationship Between Doses.” ↑
- N. K. Canby et al., “The Contribution of Common and Specific Therapeutic Factors to Mindfulness-Based Intervention Outcomes,” Frontiers in Psychology 11 (2020): 603394. ↑
- Strohmaier, “Relationship Between Doses”; A. Lloyd et al., “The Utility of Home-Practice in Mindfulness-Based Group Interventions: A Systematic Review,” Mindfulness 9, no. 3 (2018): 673–692. ↑
- A. Leyland et al., “Experimental Effects of Mindfulness Inductions on Self-Regulation: Systematic Review and Meta-Analysis,” Emotion 19, no. 1 (2019): 108–122; A. Howarth et al., “Effects of Brief Mindfulness-Based Interventions on Health-Related Outcomes: A Systematic Review,” Mindfulness 10 (2019): 1957–1968; A. S. McClintock et al., “Brief Mindfulness-Based Interventions for Acute and Chronic Pain: A Systematic Review,” Journal of Alternative and Complementary Medicine 25, no. 3 (2019): 265–278. ↑
- S. Strohmaier et al., “One-Session Mindfulness of the Breath Meditation Practice: A Randomized Controlled Study of the Effects on State Hope and State Gratitude in the General Population,” Mindfulness 13 (2022): 1–12; Leyland et al., “Experimental Effects of Mindfulness Inductions”; M. C. Schumer et al., “Brief Mindfulness Training for Negative Affectivity: A Systematic Review and Meta-Analysis,” Journal of Consulting and Clinical Psychology 86, no. 7 (2018): 569–583. ↑
- L. G. Kiken et al., “From a State to a Trait: Trajectories of State Mindfulness in Meditation During Intervention Predict Changes in Trait Mindfulness,” Personality and Individual Differences 81 (2015): 41–46; Strohmaier et al., “One-Session Mindfulness.” ↑
- J. N. Davies et al., “How Do Placebo Effects Contribute to Mindfulness-Based Analgesia? Probing Acute Pain Effects and Interactions Using a Randomized Balanced Placebo Design,” Pain 163, no. 10 (2022): 1967–1977; S. B. Goldberg, “A Common Factors Perspective on Mindfulness-Based Interventions,” Nature Reviews Psychology 1, no. 10 (2022): 605–619. ↑
- P. Grossman and N. T. van Dam, “Mindfulness, by Any Other Name . . . : Trials and Tribulations of Sati in Western Psychology and Science,” Contemporary Buddhism 12, no. 1 (2011): 219–239. ↑
- T. Brashers-Krug et al., “Consolidation in Human Motor Memory,” Nature 382, no. 6588 (1996): 252–255; E. M. Robertson et al., “Current Concepts in Procedural Consolidation,” Nature Reviews Neuroscience 5, no. 7 (2004): 576–582. ↑
- H. A. Slagter et al., “Mental Training Affects Distribution of Limited Brain Resources,” PLoS Biology 5, no. 6 (2007): e138; A. P. Zanesco et al., “Modulation of Event-Related Potentials of Visual Discrimination by Meditation Training and Sustained Attention,” Journal of Cognitive Neuroscience 31, no. 8 (2019): 1184–1204. ↑
- A. Lutz et al., “Long-Term Meditators Self-Induce High-Amplitude Gamma Synchrony During Mental Practice,” Proceedings of the National Academy of Sciences 101, no. 46 (2004): 16369–16373. ↑
- R. J. Davidson and A. W. Kaszniak, “Conceptual and Methodological Issues in Research on Mindfulness and Meditation,” American Psychologist 70, no. 7 (2015): 581–592. ↑
- J. R. Lindahl et al., “The Varieties of Contemplative Experience: A Mixed-Methods Study of Meditation-Related Challenges in Western Buddhists,” PLoS One 12, no. 5 (2017): e0176239. ↑
- S. Bostock et al., “Mindfulness On-the-Go: Effects of a Mindfulness Meditation App on Work Stress and Well-Being,” Journal of Occupational Health Psychology 24, no. 1 (2019): 127–138; J. A. M. Flett et al., “App-Based Mindfulness Meditation for Psychological Distress and Adjustment to College in Incoming University Students: A Pragmatic, Randomised, Waitlist-Controlled Trial,” Psychology & Health 35, no. 9 (2020): 1049–1074; B. L. Fredrickson et al., “Positive Emotion Correlates of Meditation Practice: A Comparison of Mindfulness Meditation and Loving-Kindness Meditation,” Mindfulness 8, no. 6 (2017): 1623–1633; J. Galante et al., “Effectiveness of Providing University Students with a Mindfulness-Based Intervention to Increase Resilience to Stress: 1-Year Follow-Up of a Pragmatic Randomised Controlled Trial,” Journal of Epidemiology and Community Health 75, no. 2 (2021): 151–160; P. L. Dobkin and Q. Zhao, “Increased Mindfulness—The Active Component of the Mindfulness-Based Stress Reduction Program?,” Complementary Therapies in Clinical Practice 17, no. 1 (2011): 22–27. ↑
- R. Gethin, The Foundations of Buddhism (Oxford University Press, 1998); D. L. McMahan, Rethinking Meditation: Buddhist Meditative Practice in Ancient and Modern Worlds (Oxford University Press, 2023). ↑
- B. Anālayo, Sattipaṭṭhāna: The Direct Path to Realization (Windhorse Publications, 2004); Bhikkhu Thanissaro, “Sona Sutta: About Sona,” Access to Insight (BCBS Edition), November 30, 2013, http://www.accesstoinsight.org/tipitaka/an/an06/an06.055.than.html. ↑
- D. T. Namgyal, Clarifying the Natural State: A Principal Guidance Manual for Mahamudra (Rangjung Yeshe Publications, 2004). ↑
- Gethin, Foundations of Buddhism; McMahan, Making of Buddhist Modernism. ↑
- E. Braun, “The Birth of Insight,” in The Birth of Insight: Modern Buddhism, and the Burmese Monk Ledi Sayadaw (University of Chicago Press, 2013). ↑
- L. Sayadaw, Manual of Mindfulness of Breathing: Ānāpāna Dīpanī, The Wheel Publication 431/432 (Buddhist Publication Society, 1999). ↑
- S. N. Goenka, Discourse Summaries (Pariyatti Publishing, 2012). ↑
- Bhikkhu Moneyya, Teaching and Training—Pa-Auk Forest Monastery (Pa-Auk Meditation Centre [Singapore], 2016). ↑
- A. Bernstein, D. R. Vago, and T. Barnhofer, “Understanding Mindfulness, One Moment at a Time: An Introduction to the Special Issue,” Current Opinion in Psychology, no. 28 (2019): vi–x; Ven. Bhikkhu Bodhi, “The Transformations of Mindfulness,” in Handbook of Mindfulness: Culture, Context, and Social Engagement, ed. R. E. Purser, D. Forbes, and A. Burke (Springer, 2016). ↑
- Goenka, Discourse Summaries; C. Titmuss, Light on Enlightenment: Revolutionary Teachings on the Inner Life (Random House, 2011); B. A. Wallace, The Attention Revolution: Unlocking the Power of the Focused Mind (Wisdom Publications, 2006). ↑
- T. N. Hanh, How to Relax (Parallax Press, 2015). ↑
- K. Witkiewitz and G. A. Marlatt, “Modeling the Complexity of Post-Treatment Drinking: It’s a Rocky Road to Relapse,” Clinical Psychology Review 27, no. 6 (2007): 724–738. ↑
- D. Winston, The Little Book of Being: Practices and Guidance for Uncovering Your Natural Awareness (Sounds True, 2019). ↑
- Goenka, Discourse Summaries; Moneyya, Teaching and Training; Wallace, Attention Revolution; J. Yates et al., The Mind Illuminated: A Complete Meditation Guide Integrating Buddhist Wisdom and Brain Science for Greater Mindfulness (Simon and Schuster, 2017). ↑
- Goenka, Discourse Summaries; H. Gunaratana, Mindfulness in Plain English (Bhavana Society, 1991); Titmuss, Light on Enlightenment; Yates et al., Mind Illuminated. ↑
- Goenka, Discourse Summaries; B. G. King et al., “Residential Meditation Retreats: Their Role in Contemplative Practice and Significance for Psychological Research,” Current Opinion in Psychology 28 (2019): 238–244; Moneyya, Teaching and Training. ↑
- Parsons et al., “Home Practice in Mindfulness-Based Cognitive Therapy.” ↑
- J. Kabat-Zinn, “An Outpatient Program in Behavioral Medicine for Chronic Pain Patients Based on the Practice of Mindfulness Meditation: Theoretical Considerations and Preliminary Results,” General Hospital Psychiatry 4, no. 1 (1982): 33–47. ↑
- Kabat-Zinn, “Some Reflections on the Origins.” ↑
- Strohmaier, “Relationship Between Doses.” ↑
- Lloyd et al., “Utility of Home-Practice.” ↑
- Sommers-Spijkerman et al., “New Evidence in the Booming Field.” ↑
- E. B. Loucks et al., “Mindfulness-Based Programs: Why, When, and How to Adapt?,” Global Advances in Health and Medicine 11 (2022). ↑
- Strohmaier, “Relationship Between Doses.” ↑
- See Loucks et al., “Mindfulness-Based Programs.” ↑
- N. I. Bowles et al., “Dose-Response Relationship of Reported Lifetime Meditation Practice with Mental-Health and Wellbeing: A Cross-Sectional Study,” Mindfulness 13 (2022): 2529–2546. ↑
- Gál et al., “Efficacy of Mindfulness Meditation Apps.” ↑
- M. T. Fish and A. D. Saul, “The Gamification of Meditation: A Randomized-Controlled Study of a Prescribed Mobile Mindfulness Meditation Application in Reducing College Students’ Depression,” Simulation & Gaming 50, no. 4 (2019): 419–435. ↑
- Anālayo, Sattipaṭṭhāna; N. Thera, The Heart of Buddhist Meditation: The Buddha’s Way to Mindfulness (Buddhist Publication Society, 2005); D. A. Rosenbaum et al., “Acquisition of Intellectual and Perceptual-Motor Skills,” Annual Review of Psychology 52, no. 1 (2001): 453–470. ↑
- Riordan et al., “How Often Should I Meditate?” ↑
- Strohmaier, “Relationship Between Doses.” ↑
- J. Masheder, L. Fjorback, and C. E. Parsons, “‘I Am Getting Something out of This, so I Am Going to Stick with It’: Supporting Participants’ Home Practice in Mindfulness-Based Programmes,” BMC Psychology 8, no. 1 (2020): 91. ↑
- J. Kabat-Zinn, Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life (Hachette Books, 2009). ↑
- H. Gunaratana, Beyond Mindfulness in Plain English: An Introductory Guide to Deeper States of Meditation, ed. J. Peddicord (Wisdom Publications, 2009); Kabat-Zinn, Wherever You Go, There You Are. ↑
- Mahasi Sayadaw, Practical Insight Meditation: Basic and Progressive Stages (Buddhist Publication Society, 1991); Yates et al., Mind Illuminated. ↑
- Y. Mingyur and E. Swanson, Joyful Wisdom (Random House, 2010). ↑
- W. B. Britton, “Can Mindfulness Be Too Much of a Good Thing? The Value of a Middle Way,” Current Opinion in Psychology 28 (2019): 159–165. ↑
- Gunaratana, Beyond Mindfulness in Plain English; Strohmaier et al., “Effects of Length of Mindfulness Practice”; J. Kabat-Zinn, Coming to Our Senses: Healing Ourselves and the World Through Mindfulness (Hachette UK, 2005). ↑
- Strohmaier et al., “Effects of Length of Mindfulness Practice”; Kabat-Zinn, Coming to Our Senses; Z. W. Adams et al., “Meditation Smartphone Application Effects on Prehypertensive Adults’ Blood Pressure: Dose-Response Feasibility Trial,” Health Psychology 37, no. 9 (2018): 850–860; Berghoff et al., “Mindfulness Meditation Adherence.” ↑
- S. L. Shapiro et al., “Mechanisms of Mindfulness,” Journal of Clinical Psychology 62, no. 3 (2006): 373–386; K. Birtwell et al., “An Exploration of Formal and Informal Mindfulness Practice and Associations with Wellbeing,” Mindfulness 10, no. 1 (2019): 89–99. ↑
- P. Lally and B. Gardner, “Promoting Habit Formation,” Health Psychology Review 7, no. S1 (2013): S137–S158. ↑
- P. Chödrön, How to Meditate (Sounds True, 2013); Gunaratana, Beyond Mindfulness in Plain English; Strohmaier et al., “Effects of Length of Mindfulness Practice”; Yates et al., Mind Illuminated. ↑
- Strohmaier, “Relationship Between Doses.” ↑
- Mingyur and Swanson, Joyful Wisdom; Winston, Little Book of Being. ↑
- Baumel et al., “Objective User Engagement.” ↑
- Goldberg et al., “Mobile Phone-Based Interventions.” ↑
- P. Sedlmeier and J. Theumer, “Why Do People Begin to Meditate and Why Do They Continue?,” Mindfulness 11, no. 6 (2020): 1527–1545. ↑
- Bowles et al., “Dose-Response Relationship”; Sedlmeier and Theumer, “Why Do People Begin.” ↑
- Bowles et al., “Dose-Response Relationship.” ↑
- Bowles et al., “Dose-Response Relationship.” ↑
- Kabat-Zinn, Coming to Our Senses. ↑
- Goenka, Discourse Summaries. ↑
- K. I. Howard et al., “The Dose-Effect Relationship in Psychotherapy,” American Psychologist 41, no. 2 (1986): 159–164. ↑
- Bowles et al., “Dose-Response Relationship.” ↑
- Gál et al., “Efficacy of Mindfulness Meditation Apps”; Supplementary Files, https://osf.io/6wpa3/overview. ↑
- See, e.g., G. Desbordes et al., “Moving Beyond Mindfulness: Defining Equanimity as an Outcome Measure in Meditation and Contemplative Research,” Mindfulness 6 (2014): 356–372; B. K. Hölzel et al., “How Does Mindfulness Meditation Work? Proposing Mechanisms of Action from a Conceptual and Neural Perspective,” Perspectives on Psychological Science 6, no. 6 (2011): 537–559; Shapiro et al., “Mechanisms of Mindfulness.” ↑
- A. Nwosu et al., “Digital Therapeutics for Mental Health: Is Attrition the Achilles Heel?,” Frontiers in Psychiatry 13 (2022): 1598. ↑
- Adams et al., “Meditation Smartphone Application Effects”; Berghoff et al., “Mindfulness Meditation Adherence.” ↑
- See, e.g., Baumel et al., “Objective User Engagement.” ↑
- Birtwell et al., “Exploration of Formal and Informal.” ↑
- See, e.g., C. Ye et al., “Estimating Treatment Effects in Randomised Controlled Trials with Non-Compliance: A Simulation Study,” BMJ Open 4, no. 6 (2014): e005362. ↑
- See, e.g., M. A. Hernán and J. M. Robins, “Per-Protocol Analyses of Pragmatic Trials,” New England Journal of Medicine 377, no. 14 (2017): 1391–1398. ↑
- J. Cook and J. Cassaniti, “Mindfulness and Culture,” Anthropology Today 38, no. 2 (2022): 1–3; E. Thompson, Why I Am Not a Buddhist (Yale University Press, 2020). ↑
- Bodhi, “Transformations of Mindfulness.” ↑
- Supplementary Files, https://osf.io/6wpa3/overview. ↑
- Supplementary Files, https://osf.io/6wpa3/overview. ↑
- T. Brach, “How to Meditate FAQ: A Definitive Guide to a Gratifying Practice,” effective February 6, 2016, https://www.tarabrach.com/wp-content/uploads/pdf/How-to-Meditate–FAQ.pdf. ↑
- P. Chödrön, How to Meditate, 15. ↑
- C. Feldman, 20 Minutes to Master Meditation (HarperCollins, 1998). ↑
- “3 Ways to Build a Sustainable Meditation Practice,” Mindful, effective March 3, 2017, https://www.mindful.org/3-ways-build-sustainable-meditation-practice/. ↑
- T. N. Hanh, The Miracle of Mindfulness (Random House, 2008), 31. ↑
- J. Kabat-Zin, interviewed by Maia Szalavitz, “Q&A: Jon Kabat-Zinn Talks About Bringing Mindfulness Meditation to Medicine,” TIME Healthland, January 12, 2012, https://healthland.time.com/2012/01/11/mind-reading-jon-kabat-zinn-talks-about-bringing-mindfulness-meditation-to-medicine/. ↑
- Kabat-Zinn, Wherever You Go, There You Are, 126. ↑
- J. Kornfield, The Wise Heart: Buddhist Psychology for the West (Random House, 2008), 84. ↑
- Gunaratana, Mindfulness in Plain English, 45. ↑
- K. McDonald, How to Meditate: A Practical Guide (Simon and Schuster, 2005), 15. ↑
- Tergar, “Meditation FAQ,” 2012, https://tergar.org/meditation/. ↑
- W. Rāhula, What the Buddha Taught (Grove Press, 1974), 70. ↑
- M. Ricard, The Art of Meditation (Atlantic Books Ltd., 2010), 14. ↑
- L. Rosenberg, Breath by Breath: The Liberating Practice of Insight Meditation (Shambhala Publications, 2004), 179. ↑
- S. Salzberg, “Just Sit,” O Magazine, November 1, 2002, https://www.sharonsalzberg.com/just-sit/. ↑
- Ajahn Sumedho, Mindfulness—The Path of the Deathless (Amaravati Publications, 1987), 26. ↑
- Titmuss, Light on Enlightenment, 54. ↑
- C. Trungpa, Mindfulness in Action: Making Friends with Yourself Through Meditation and Everyday Awareness (Shambhala Publications, 2015), 24–25. ↑
- Wallace, Attention Revolution, 21. ↑
- Winston, Little Book of Being, 66. ↑
- Yates et al., Mind Illuminated, 114. ↑
Works Cited
Adams, Z. W., J. C. Sieverdes, B. Brunner-Jackson, et al. “Meditation Smartphone Application Effects on Prehypertensive Adults’ Blood Pressure: Dose-Response Feasibility Trial.” Health Psychology 37, no. 9 (2018): 850–860. https://doi.org/10.1037/hea0000584. Anālayo, B. Sattipaṭṭhāna: The Direct Path to Realization. Windhorse Publications, 2004.
Baumel, A., F. Muench, S. Edan, and J. M. Kane. “Objective User Engagement with Mental Health Apps: Systematic Search and Panel-Based Usage Analysis.” Journal of Medical Internet Research 21, no. 9 (2019): e14567. https://doi.org/10.2196/14567.
Berghoff, C. R., L. E. Wheeless, T. R. Ritzert, C. M. Wooley, and J. P. Forsyth. “Mindfulness Meditation Adherence in a College Sample: Comparison of a 10-Min versus 20-Min 2-Week Daily Practice.” Mindfulness 8, no. 6 (2017): 1513–1521. https://doi.org/10.1007/s12671-017-0717-y.
Bernstein, A., D. R. Vago, and T. Barnhofer. “Understanding Mindfulness, One Moment at a Time: An Introduction to the Special Issue.” Current Opinion in Psychology 28 (2019): vi–x. https://doi.org/10.1016/j.copsyc.2019.08.001.
Birtwell, K., K. Williams, H. van Marwijk, C. J. Armitage, and D. Sheffield. “An Exploration of Formal and Informal Mindfulness Practice and Associations with Wellbeing.” Mindfulness 10, no. 1 (2019): 89–99. https://doi.org/10.1007/s12671-018-0951-y.
Bodhi, Ven. Bhikkhu. “The Transformations of Mindfulness.” In Handbook of Mindfulness: Culture, Context, and Social Engagement, edited by R. E. Purser, D. Forbes, and A. Burke. Springer, 2016. https://doi.org/10.1007/978-3-319-44019-4_1.
Bostock, S., A. D. Crosswell, A. A. Prather, and A. Steptoe. “Mindfulness On-the-Go: Effects of a Mindfulness Meditation App on Work Stress and Well-Being.” Journal of Occupational Health Psychology 24, no. 1 (2019): 127–138. https://doi.org/10.1037/ocp0000118.
Bowles, N. I., J. N. Davies, and N. T. van Dam. “Dose-Response Relationship of Reported Lifetime Meditation Practice with Mental-Health and Wellbeing: A Cross-Sectional Study.” Mindfulness 13 (2022): 2529–2546. https://doi.org/10.1007/s12671-022-01977-6.
Brashers-Krug, T., R. Shadmehr, and E. Bizzi. “Consolidation in Human Motor Memory.” Nature 382, no. 6588 (1996): 252–255. https://doi.org/10.1038/382252a0.
Brach, T. “How to Meditate FAQ: A Definitive Guide to a Gratifying Practice.” Effective February 6, 2016. https://www.tarabrach.com/wp-content/uploads/pdf/How-to-Meditate–FAQ.pdf.
Braun, E. “The Birth of Insight.” In The Birth of Insight: Meditation, Modern Buddhism, and the Burmese Monk Ledi Sayadaw. University of Chicago Press, 2013.
Britton, W. B. “Can Mindfulness Be Too Much of a Good Thing? The Value of a Middle Way.” Current Opinion in Psychology 28 (2019): 159–165. https://doi.org/10.1016/j.copsyc.2018.12.011
Canby, N. K., K. Eichel, J. Lindahl, S. Chau, J. Cordova, and W. B. Britton. “The Contribution of Common and Specific Therapeutic Factors to Mindfulness-Based Intervention Outcomes.” Frontiers in Psychology 11 (2020): 603394. https://doi.org/10.3389/fpsyg.2020.603394.
Chödrön, P. How to Meditate: A Practical Guide to Making Friends with Your Mind. Sounds True, 2013.
Cook, J., and J. Cassaniti. “Mindfulness and Culture.” Anthropology Today 38, no. 2 (2022): 1–3. https://doi.org/10.1111/1467-8322.12704.
Crane, R. S., J. Brewer, C. Feldman, et al. “What Defines Mindfulness-Based Programs? The Warp and the Weft.” Psychological Medicine 47, no. 6 (2017): 990–999. https://doi.org/10.1017/S0033291716003317.
Davidson, R. J. and A. W. Kaszniak. “Conceptual and Methodological Issues in Research on Mindfulness and Meditation.” American Psychologist 70, no. 7 (2015): 581–592. https://doi.org/10.1037/a0039512.
Davies, J. N., A. Faschinger, J. Galante, and N. T. Van Dam. “Prevalence and 20-Year Trends in Meditation, Yoga, Guided Imagery and Progressive Relaxation Use Among US Adults from 2002 to 2022.” Scientific Reports 14, no. 1 (2024): 14987. https://doi.org/10.1038/s41598-024-64562-y.
Davies, J. N., L. Sharpe, M. A. Day, and B. Colagiuri. “How Do Placebo Effects Contribute to Mindfulness-Based Analgesia? Probing Acute Pain Effects and Interactions Using a Randomized Balanced Placebo Design.” Pain 163, no. 10 (2022): 1967–1977. https://doi.org/10.1097/j.pain.0000000000002593.
Desbordes, G., T. Gard, E. A. Hoge, et al. “Moving Beyond Mindfulness: Defining Equanimity as an Outcome Measure in Meditation and Contemplative Research.” Mindfulness 6 (2014): 356–372. https://doi.org/10.1007/s12671-013-0269-8.
Dobkin, P. L., and Q. Zhao. “Increased Mindfulness—The Active Component of the Mindfulness-Based Stress Reduction Program?” Complementary Therapies in Clinical Practice 17, no. 1 (2011): 22–27. https://doi.org/10.1016/j.ctcp.2010.03.002.
Feldman, C. 20 Minutes to Master Meditation. HarperCollins, 1998.
Fincham, G. W., K. Mavor, and B. Dritschel. “Effects of Mindfulness Meditation Duration and Type on Well-Being: An Online Dose-Ranging Randomized Controlled Trial.” Mindfulness 14 (2023): 1171–1182. https://doi.org/10.1007/s12671-023-02119-2.
Fish, M. T., and A. D. Saul. “The Gamification of Meditation: A Randomized-Controlled Study of a Prescribed Mobile Mindfulness Meditation Application in Reducing College Students’ Depression.” Simulation & Gaming 50, no. 4 (2019): 419–435. https://doi.org/10.1177/1046878119851821.
Flett, J. A. M., T. S. Conner, B. C. Riordan, T. Patterson, and H. Hayne. “App-Based Mindfulness Meditation for Psychological Distress and Adjustment to College in Incoming University Students: A Pragmatic, Randomised, Waitlist-Controlled Trial.” Psychology & Health 35, no. 9 (2020): 1049–1074. https://doi.org/10.1080/08870446.2019.1711089.
Fredrickson, B. L., A. J. Boulton, A. M. Firestine, et al. “Positive Emotion Correlates of Meditation Practice: A Comparison of Mindfulness Meditation and Loving-Kindness Meditation.” Mindfulness 8, no. 6 (2017): 1623–1633. https://doi.org/10.1007/s12671-017-0735-9.
Gál, É., S. Ștefan, and I. A. Cristea. “The Efficacy of Mindfulness Meditation Apps in Enhancing Users’ Well-Being and Mental Health Related Outcomes: A Meta-Analysis of Randomized Controlled Trials.” Journal of Affective Disorders 279 (2021): 131–142. https://doi.org/10.1016/j.jad.2020.09.134/
Galante, J., C. Friedrich, A. F. Dawson, et al. “Mindfulness-Based Programmes for Mental Health Promotion in Adults in Nonclinical Settings: A Systematic Review and Meta-Analysis of Randomised Controlled Trials.” PLoS Medicine 18, no. 1 (2021): e1003481. https://doi.org/10.1371/journal.pmed.1003481.
Galante, J., J. Stochl, G. Dufour, M. Vainre, A. P. Wagner, and P. B. Jones. “Effectiveness of Providing University Students with a Mindfulness-Based Intervention to Increase Resilience to Stress: 1-Year Follow-Up of a Pragmatic Randomised Controlled Trial.” Journal of Epidemiology and Community Health 75, no. 2 (2021): 151–160. https://doi.org/10.1136/jech-2020-214390.
Gethin, R. The Foundations of Buddhism. Oxford University Press, 1998.
Goenka, S. N. Discourse Summaries. Pariyatti Publishing, 2012.
Goldberg, S. B. “A Common Factors Perspective on Mindfulness-Based Interventions.” Nature Reviews Psychology 1, no. 10 (2022): 605–619. https://doi.org/10.1038/s44159-022-00090-8.
Goldberg, S. B., A. D. Kendall, M. J. Hirshberg, et al. “Is Dosage of a Meditation App Associated with Changes in Psychological Distress? It Depends on How You Ask.” Clinical Psychological Science 13, no. 2 (2024): 332–349. https://doi.org/10.1177/21677026241266567.
Goldberg, S. B., S. U. Lam, O. Simonsson, J. Torous, and S. Sun. “Mobile Phone-Based Interventions for Mental Health: A Systematic Meta-Review of 14 Meta-Analyses of Randomized Controlled Trials.” PLOS Digital Health 1, no. 1 (2022): e0000002. https://doi.org/10.1371/journal.pdig.0000002.
Grossman, P., and N. T. van Dam. “Mindfulness, by Any Other Name . . . : Trials and Tribulations of Sati in Western Psychology and Science.” Contemporary Buddhism 12, no. 1 (2011): 219–239. https://doi.org/10.1080/14639947.2011.564841.
Gunaratana, H. Beyond Mindfulness in Plain English: An Introductory Guide to Deeper States of Meditation. Edited by John Peddicord. Wisdom Publications, 2009.
Gunaratana, H. Mindfulness in Plain English. Bhavana Society, 1991.
Hanh, T. N. How to Relax. Parallax Press, 2015. Hanh, T. N. The Miracle of Mindfulness. Random House, 2008.
Hernán, M. A., and J. M. Robins. “Per-Protocol Analyses of Pragmatic Trials.” New England Journal of Medicine 377, no. 14 (2017): 1391–1398. https://doi.org/10.1056/NEJMsm1605385.
Hölzel, B. K., S. W. Lazar, T. Gard, Z. Schuman-Olivier, D. R. Vago, and U. Ott. “How Does Mindfulness Meditation Work? Proposing Mechanisms of Action from a Conceptual and Neural Perspective.” Perspectives on Psychological Science 6, no. 6 (2011): 537–559. https://doi.org/10.1177/1745691611419671.
Howard, K. I., S. M. Kopta, M. S. Krause, and D. E. Orlinsky. “The Dose-Effect Relationship in Psychotherapy.” American Psychologist 41, no. 2 (1986): 159–164. https://doi.org/10.1037/0003-066X.41.2.159.
Howarth, A., J. G. Smith, L. Perkins-Porras, and M. Ussher. “Effects of Brief Mindfulness-Based Interventions on Health-Related Outcomes: A Systematic Review.” Mindfulness 10 (2019): 1957–1968. https://doi.org/10.1007/s12671-019-01163-1.
Kabat-Zinn, J. “An Outpatient Program in Behavioral Medicine for Chronic Pain Patients Based on the Practice of Mindfulness Meditation: Theoretical Considerations and Preliminary Results.” General Hospital Psychiatry 4, no. 1 (1982): 33–47. https://doi.org/10.1016/0163-8343(82)90026-3.
Kabat-Zinn, J. Coming to Our Senses: Healing Ourselves and the World Through Mindfulness. Hachette UK, 2005.
Kabat-Zinn, J. “Q&A: Jon Kabat-Zinn Talks About Bringing Mindfulness Meditation to Medicine.” Interviewed by M. Szalavitz. TIME Healthland, January 12, 2012. https://healthland.time.com/2012/01/11/mind-reading-jon-kabat-zinn-talks-about-bringing-mindfulness-meditation-to-medicine/.
Kabat-Zinn, J. “Some Reflections on the Origins of MBSR, Skillful Means, and the Trouble with Maps.” Contemporary Buddhism 12, no. 1 (2011): 281–306. https://doi.org/10.1080/14639947.2011.564844.
Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life. Hachette Books, 2009.
Kiken, L. G., E. L. Garland, K. Bluth, O. S. Palsson, and S. A. Gaylord. “From a State to a Trait: Trajectories of State Mindfulness in Meditation During Intervention Predict Changes in Trait Mindfulness.” Personality and Individual Differences 81 (2015): 41–46. https://doi.org/10.1016/j.paid.2014.12.044.
King, B. G., Q. A. Conklin, A. P. Zanesco, and C. D. Saron. “Residential Meditation Retreats: Their Role in Contemplative Practice and Significance for Psychological Research.” Current Opinion in Psychology 28 (2019): 238–244. https://doi.org/10.1016/j.copsyc.2018.12.021.
Kornfield, J. The Wise Heart: Buddhist Psychology for the West. Random House, 2008.
Lally, P., and B. Gardner. “Promoting Habit Formation.” Health Psychology Review 7, no. S1 (2013): S137–S158. https://doi.org/10.1080/17437199.2011.603640.
Leyland, A., G. Rowse, and L. Emerson. “Experimental Effects of Mindfulness Inductions on Self-Regulation: Systematic Review and Meta-Analysis.” Emotion 19, no. 1 (2019): 108–122. https://doi.org/10.1037/emo0000425.
Lindahl, J. R., N. E. Fisher, D. J. Cooper, R. K. Rosen, and W. B. Britton. “The Varieties of Contemplative Experience: A Mixed-Methods Study of Meditation-Related Challenges in Western Buddhists.” PLoS One 12, no. 5 (2017): e0176239. https://doi.org/10.1371/journal.pone.0176239.
Lloyd, A., R. White, C. Eames, and R. Crane. “The Utility of Home-Practice in Mindfulness-Based Group Interventions: A Systematic Review.” Mindfulness 9, no. 3 (2018): 673–692. https://doi.org/10.1007/s12671-017-0813-z.
Loucks, E. B., R. S. Crane, M. A. Sanghvi, et al. “Mindfulness-Based Programs: Why, When, and How to Adapt?” Global Advances in Health and Medicine 11 (2022). https://doi.org/10.1177/21649561211068805.
Lutz, A., L. L. Greischar, N. B. Rawlings, M. Ricard, and R. J. Davidson. “Long-Term Meditators Self-Induce High-Amplitude Gamma Synchrony During Mental Practice.” Proceedings of the National Academy of Sciences 101, no. 46 (2004): 16369–16373. https://doi.org/10.1073/pnas.0407401101.
Masheder, J., L. Fjorback, and C. E. Parsons. “‘I Am Getting Something out of This, so I Am Going to Stick with It’: Supporting Participants’ Home Practice in Mindfulness-Based Programmes.” BMC Psychology 8, no. 1 (2020): 91. https://doi.org/10.1186/s40359-020-00453-x.
McClintock, A. S., S. M. McCarrick, E. L. Garland, F. Zeidan, and A. E. Zgierska. “Brief Mindfulness-Based Interventions for Acute and Chronic Pain: A Systematic Review.” Journal of Alternative and Complementary Medicine 25, no. 3 (2019): 265–278. https://doi.org/10.1089/acm.2018.0351.
McDonald, K. How to Meditate: A Practical Guide. Simon and Schuster, 2005.
McMahan, D. L. The Making of Buddhist Modernism. Oxford University Press, 2008.
McMahan, D. L. Rethinking Meditation: Buddhist Meditative Practice in Ancient and Modern Worlds. Oxford University Press, 2023.
Mindful. “3 Ways to Build a Sustainable Meditation Practice.” Effective March 3, 2017. https://www.mindful.org/3-ways-build-sustainable-meditation-practice/.
Mingyur, Y., and E. Swanson. Joyful Wisdom. Random House, 2010.
Moneyya, Bhikkhu. Teaching and Training—Pa-Auk Forest Monastery. Pa-Auk Meditation Centre (Singapore), 2016.
Namgyal, D. T. Clarifying the Natural State: A Principal Guidance Manual for Mahamudra. Rangjung Yeshe Publications, 2004.
Nwosu, A., S. Boardman, M. M. Husain, and P. M. Doraiswamy. “Digital Therapeutics for Mental Health: Is Attrition the Achilles Heel?” Frontiers in Psychiatry 13 (2022): 1598. https://doi.org/10.3389/fpsyt.2022.900615.
Palmer, R., C. Roos, N. Vafaie, and H. Kober. “The Effect of Ten versus Twenty Minutes of Mindfulness Meditation on State Mindfulness and Affect.” Scientific Reports 13, no. 1 (2023): 20646. https://doi.org/10.1038/s41598-023-46578-y.
Parsons, C. E., C. Crane, L. J. Parsons, L. O. Fjorback, and W. Kuyken. “Home Practice in Mindfulness-Based Cognitive Therapy and Mindfulness-Based Stress Reduction: A Systematic Review and Meta-Analysis of Participants’ Mindfulness Practice and Its Association with Outcomes.” Behaviour Research and Therapy 95 (2017): 29–41. https://doi.org/10.1016/j.brat.2017.05.004.
Rāhula, W. What the Buddha Taught. Grove Press, 1974. Ricard, M. The Art of Meditation. Atlantic Books Ltd., 2010.
Riordan, K. M., O. Simonsson, C. Frye, et al. “How Often Should I Meditate? A Randomized Trial Examining the Role of Meditation Frequency When Total Amount of Meditation Is Held Constant.” Journal of Counseling Psychology 71, no. 2 (2024): 104–114. https://doi.org/10.1037/cou0000725.
Robertson, E. M., A. Pascual-Leone, and R. C. Miall. “Current Concepts in Procedural Consolidation.” Nature Reviews Neuroscience 5, no. 7 (2004): 576–582. https://doi.org/10.1038/nrn1426.
Rosenbaum, D. A., R. A. Carlson, and R. O. Gilmore. “Acquisition of Intellectual and Perceptual-Motor Skills.” Annual Review of Psychology 52, no. 1 (2001): 453–470. https://doi.org/10.1146/annurev.psych.52.1.453.
Rosenberg, L. Breath by Breath: The Liberating Practice of Insight Meditation. Shambhala Publications, 2004. Salzberg, S. “Just Sit.” O Magazine, November 1, 2002. https://www.sharonsalzberg.com/just-sit/.
Sayadaw, L. Manual of Mindfulness of Breathing: Ānāpāna Dīpanī. The Wheel Publication 431/432. Buddhist Publication Society, 1999.
Sayadaw, Mahasi. Practical Insight Meditation: Basic and Progressive Stages. Buddhist Publication Society, 1991.
Schumer, M. C., E. K. Lindsay, and J. D. Creswell. “Brief Mindfulness Training for Negative Affectivity: A Systematic Review and Meta-Analysis.” Journal of Consulting and Clinical Psychology 86, no. 7 (2018): 569–583. https://doi.org/10.1037/ccp0000324.
Sedlmeier, P., and J. Theumer. “Why Do People Begin to Meditate and Why Do They Continue?” Mindfulness 11, no. 6 (2020): 1527–1545. https://doi.org/10.1007/s12671-020-01367-w.
Shapiro, S. L., L. E. Carlson, J. A. Astin, and B. Freedman. “Mechanisms of Mindfulness.” Journal of Clinical Psychology 62, no. 3 (2006): 373–386. https://doi.org/10.1002/jclp.20237.
Simonsson, O., S. Fisher, and M. Martin. “Awareness and Experience of Mindfulness in Britain.” Sociological Research Online 26, no. 4 (2021): 833–852. https://journals.sagepub.com/doi/10.1177/1360780420980761.
Slagter, H. A., A. Lutz, L. L. Greischar, et al. “Mental Training Affects Distribution of Limited Brain Resources.” PLoS Biology 5, no. 6 (2007): e138. https://doi.org/10.1371/journal.pbio.0050138.
Sommers-Spijkerman, M., J. Austin, E. Bohlmeijer, and W. Pots. “New Evidence in the Booming Field of Online Mindfulness: An Updated Meta-Analysis of Randomized Controlled Trials.” JMIR Mental Health 8, no. 7 (2021): e28168. https://doi.org/10.2196/28168.
Strohmaier, S. “The Relationship Between Doses of Mindfulness-Based Programs and Depression, Anxiety, Stress, and Mindfulness: A Dose-Response Meta-Regression of Randomized Controlled Trials.” Mindfulness 11 (2020): 1315–1335. https://doi.org/10.1007/s12671-020-01319-4.
Strohmaier, S., F. W. Jones, and J. E. Cane. “Effects of Length of Mindfulness Practice on Mindfulness, Depression, Anxiety, and Stress: A Randomized Controlled Experiment.” Mindfulness 12 (2021): 198–214. https://doi.org/10.1007/s12671-020-01512-5.
Strohmaier, S., F. W. Jones, and J. E. Cane. “One-Session Mindfulness of the Breath Meditation Practice: A Randomized Controlled Study of the Effects on State Hope and State Gratitude in the General Population.” Mindfulness 13 (2022): 1–12. https://doi.org/10.1007/s12671-021-01780-9.
Sumedho, A. Mindfulness: The Path of the Deathless. Amaravati Publications, 1987.
Sylvia, L. G., N. J. French, N. George, et al. Comparing Standard and Short Online Mindfulness Therapy Programs for Improving Well-Being—The Healthy Mind Healthy You Study. Patient-Centered Outcomes Research Institute (PCORI), 2022. https://doi.org/10.25302/05.2022.XPPRN.151233786.
Tergar. “Meditation FAQ.” 2012. https://tergar.org/meditation/.
Thanissaro, Bhikkhu. “Sona Sutta: About Sona.” Access to Insight (BCBS Edition), November 30, 2013. http://www.accesstoinsight.org/tipitaka/an/an06/an06.055.than.html.
Thera, N. The Heart of Buddhist Meditation: The Buddha’s Way to Mindfulness. Buddhist Publication Society, 2005.
Thompson, E. Why I Am Not a Buddhist. Yale University Press, 2020.
Titmuss, C. Light on Enlightenment: Revolutionary Teachings on the Inner Life. Random House, 2011. Trungpa, C. Mindfulness in Action: Making Friends with Yourself Through Meditation and Everyday Awareness. Shambhala Publications, 2015.
Van Dam, N. T., M. K. van Vugt, D. R. Vago, et al. “Mind the Hype: A Critical Evaluation and Prescriptive Agenda for Research on Mindfulness and Meditation.” Perspectives on Psychological Science 13, no. 1 (2018): 36–61. https://doi.org/10.1177/1745691617709589.
Wallace, B. A. The Attention Revolution: Unlocking the Power of the Focused Mind. Wisdom Publications, 2006.
Winston, D. The Little Book of Being: Practices and Guidance for Uncovering Your Natural Awareness. Sounds True, 2019.
Witkiewitz, K., and G. A. Marlatt. “Modeling the Complexity of Post-Treatment Drinking: It’s a Rocky Road to Relapse.” Clinical Psychology Review 27, no. 6 (2007): 724–738. https://doi.org/10.1016/j.cpr.2007.01.002.
Yates, J., M. Immergut, and J. Graves. The Mind Illuminated: A Complete Meditation Guide Integrating Buddhist Wisdom and Brain Science for Greater Mindfulness. Simon and Schuster, 2017.
Ye, C., J. Beyene, G. Browne, and L. Thabane. “Estimating Treatment Effects in Randomised Controlled Trials with Non-Compliance: A Simulation Study.” BMJ Open 4, no. 6 (2014): e005362. https://doi.org/10.1136/bmjopen-2014-005362.
Zanesco, A. P., B. G. King, C. Powers, et al. “Modulation of Event-Related Potentials of Visual Discrimination by Meditation Training and Sustained Attention.” Journal of Cognitive Neuroscience 31, no. 8 (2019): 1184–1204. https://doi.org/10.1162/jocn_a_01419.
About this Article
Authors
Published February 12, 2026
Cite As
License
All JCS articles are available under a CC BY-NC-ND 4.0 license.